Praca poglądowa | Review paper
The role of platelet-rich plasma in pressure ulcer healing: a narrative review of the available literature
Dorota Trzeciak ![]() 1, Karolina Kruszewska-Bąk
1, Karolina Kruszewska-Bąk ![]() 2, Katarzyna Wesołowska-Górniak
2, Katarzyna Wesołowska-Górniak ![]() 2
2
1 Podos Wound Care Clinic, Warsaw, Poland
2 Department of Clinical Nursing, Medical University of Warsaw, Poland
Address for correspondence
Karolina Kruszewska-Bąk, Department of Clinical Nursing, Medical
University of Warsaw, 27 Erazma Ciołka St, 01-445 Warsaw, Poland,
e-mail: karolina.kruszewska@wum.edu.pl
Received: 06.0.12026 Accepted: 26.02.2026
LECZENIE RAN 2025; 22 (4): 169-176
DOI: https://doi.org/10.60075/lr.v22i3.144
Table of contents:
Abstract
Introduction
Forms of platelet-rich plasma and methods of obtaining it
Aim of the study
Material and methods
Results
Discussion
Conclusions
Disclosures
References
Abstract
Introduction: Chronic wounds, such as pressure ulcers, venous leg ulcers or diabetic foot ulcers represent a significant economic, social, and health burden on society. This burden is growing rapidly as populations in developing countries age. The most common problems in chronic wound treatment include microcirculation disorders, chronic inflammation, impaired angiogenesis, insufficient proliferation of fibroblasts and keratinocytes, and comorbidities such as diabetes or immobilization. In recent years, there has been growing interest in the use of platelet-rich plasma (PRP) for the treatment of chronic wounds of various etiologies, including pressure ulcers. This study aims to analyze the current literature on the use of PRP as an adjunctive therapy for treating pressure ulcers, emphasizing its therapeutic effects, potential problems, and limitations.
Material and methods: A narrative review of the literature on using PRP to treat pressure ulcers in adults was conducted using the PubMed and Scopus databases. The following keywords were used in the search: “platelet-rich plasma,” “PRP,” “chronic wounds,” “pressure ulcer,” and “pressure injuries.” The literature search was limited to randomized controlled trials published between 2020 and 2025. A total of 53 records were identified. After removing two duplicates, 51 articles were selected for preliminary analysis. Forty-eight studies were excluded based on their titles and abstracts. Three studies on pressure ulcers treatment procedures in adults were included in this review. The selection process occurred in two stages: first, the titles and abstracts were analyzed; then, the full texts were examined.
Results: A review of literature on PRP therapy for pressure ulcers revealed that this method supports the wound healing process, reduces wound surface area, and leads to complete healing while shortening treatment time. PRP therapy is a safe method with no reported complications.
Conclusions: Using PRP for local wound treatment may reduce healing time, thereby decreasing healthcare costs for patients with hard-to-heal wounds. Further multicenter studies are required to confirm the method’s effectiveness.
Key words: platelet-rich plasma, PRP, chronic wound, pressure ulcer, pressure injury.
Introduction
Chronic wounds, such as diabetic foot ulcers, venous leg ulcers, and pressure ulcers, represent a significant economic, social, and health burden on society, which is rapidly increasing with the ageing of the population in developing countries [1].
The physiological wound healing process involves three phases: inflammation, tissue formation, and tissue remodeling. Normal wound healing involves a series of complex biological and molecular processes, including cell migration and proliferation, synthesis and deposition of the extracellular matrix, and vascularization and remodeling [1, 2]. However, in chronic wounds, these phases are inhibited, particularly proliferation and matrix remodeling.
These phases require cell migration to form granulation tissue and epithelialization [1–3]. The epithelialization process is impaired in all types of chronic wounds. Restoring regular blood supply creates a favorable microenvironment for the migration and proliferation of epidermal and dermal cells. This, in turn, leads to wound re-epithelialization and restoration of epidermal integrity [1, 3].
Despite advances in modern dressings, surgical techniques, and supportive therapies, a significant proportion of wounds fail to heal within the expected timeframe. This can lead to prolonged treatment, recurrence, and infectious complications, as well as a deterioration in patients’ quality of life. The most common problems in chronic wound treatment include microcirculation disorders, chronic inflammation, impaired angiogenesis, insufficient proliferation of fibroblasts and keratinocytes, and comorbidities such as diabetes, chronic venous insufficiency, and immobilization [1, 4]. Uncontrolled diabetes increases oxidative stress by elevating levels of advanced glycation end products, thereby impairing wound healing processes [5]. Additionally, immune deficiency, malnutrition, and certain medications, such as corticosteroids, may also hinder wound healing [2].
Regardless of the etiology of the wound, effective treatment requires the creation of an appropriate microenvironment conducive to tissue regeneration. Standard procedures include wound cleansing, infection control, offloading or compression therapy, and the appropriate selection of dressings. More advanced wound treatment methods are also available, such as revascularization, skin grafts, and vacuum-assisted closure (VAC) [2, 6]. However, in many cases, these measures prove insufficient, prompting the search for adjunctive therapies that can modulate the impaired healing process [3–7].
One promising area of biological therapy is the use of platelet-rich plasma (PRP), a treatment method recognized in medicine since the 1980s [8]. In recent years, platelet concentrates have gained widespread acceptance as an adjunctive therapy for both acute and chronic wounds [8, 9].
These concentrates can stimulate the supraphysiological release of various bioactive factors, including growth factors, cytokines, and chemokines. These factors act at different stages of wound healing through endocrine, paracrine, and autocrine mechanisms. Additionally, the neutrophils and macrophages present in platelet concentrates play a pivotal role in combating microorganisms and clearing away cellular debris [9].
Platelet-rich plasma is an autologous serum obtained from whole blood by centrifugation. It contains high concentrations of platelets, growth factors, and cytokines, which promote stem cell regeneration and tissue remodeling [10]. The platelet concentration in plasma is higher than the initial concentration, ranging from 150 × 10³/dl to 400 × 10³/dl, which is 4–5 times higher than in whole blood [11]. The classic PRP preparation method consists of two steps. First, the blood is centrifuged to separate the components into three layers: red blood cells, a transparent layer containing most of the platelets and white blood cells, and low-quality platelet plasma. The second step involves collecting the concentrated platelets in a small volume of plasma, known as PRP [11].
As an adjunctive therapy, PRP may reduce ulcer-healing time, thereby improving patients’ quality of life and alleviating the burden on the healthcare system associated with wound care [10, 12]. In recent years, there has been growing interest in the use of PRP for the treatment of chronic wounds of various etiologies, including diabetic foot ulcers, venous leg ulcers, and pressure ulcers. However, despite numerous clinical reports, the efficacy of PRP, the optimal protocols for its use, and the potential limitations of this approach remain subjects of debate.
Platelet-rich plasma is a concentrated preparation of platelets suspended in a small volume of plasma that supports the wound healing process. Platelet-rich plasma is prepared by collecting autologous blood from the patient and subsequently centrifuging it to separate platelets from other blood components. To be classified as “platelet-rich,” the platelet concentration must be at least five times higher than the baseline level in whole blood [5]. Given that the average platelet count in healthy individuals is approximately 200,000 ±75,000 per µl, a concentration of 1 million platelets per µl in PRP is considered the optimal therapeutic dose [2].
Platelet-rich plasma therapy fosters a biological environment that promotes tissue homeostasis restoration. This effect is achieved through the delivery of numerous signaling cytokines and growth factors that play a crucial role in tissue repair via multiple mechanisms, including the regulation of inflammation, angiogenesis, and new tissue synthesis and remodeling [13].
Platelet-rich plasma contains a high concentration of thrombocytes and platelet α-granules, which release numerous growth factors. The release of these factors is caused by platelet degranulation by proteins such as thrombin. These include platelet-derived growth factor, transforming growth factor β1 and β2, platelet factor IV, interleukin-1, vascular-endothelial growth factor, epidermal growth factor, insulin-like growth factor, osteocalcin, osteonectin, fibrinogen, vitronectin, fibronectin, and thrombospondin-1 [14, 15]. These factors stimulate cell proliferation and differentiation, leading to tissue formation.
Various protocols enable the preparation of PRP with different concentrations of platelets, leukocytes, and growth factors [5, 13].
The most popular technique is to take a blood sample from the patient themselves (autologous). This blood is then centrifuged to separate the platelets from the red and white blood cells. The resulting growth factor-rich platelets are highly concentrated and suspended in a small volume of plasma. Although PRP activation is not mandatory, adding thrombin and calcium chloride can enhance it by promoting the release of growth factors and bioactive proteins from platelet alpha granules.
Forms of platelet-rich plasma and methods of obtaining it
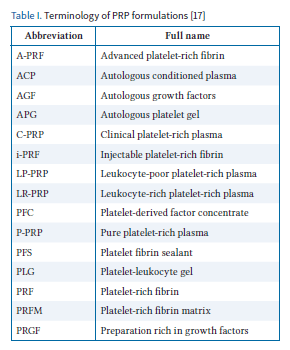
Based on its cellular components and fibrin structure, PRP can be divided into four main categories: pure PRP (P-PRP), plasma rich in leukocytes and platelets (L-PRP), pure PRF (P-PRF), and L-PRF [16]. Unfortunately, the literature often lacks standardized terminology for PRP products. Some authors define PRP as containing only platelets, while others note that it also includes increased concentrations of red blood cells, white blood cells of various types, fibrin, and bioactive proteins [17]. Table I shows the terminology and abbreviations of PRP formulations.
The products of PRP can be applied topically as a gel or injected intradermally into the edges and center of a wound [16]. The different forms of PRP are shown in Figures 1 and 2.
The topical application of homologous PRP gel to non-healing wounds favorably reduces wound size and induces granulation tissue formation. The PRP gel can be applied to the wound once or twice a week [5]. Various protocols describe the speed, time, temperature of centrifugation, and the type of anticoagulant used in PRP preparation. These differences affect the yield of bioactive material, making it difficult to compare efficacy [18]. The most common method of preparing PRP involves collecting a whole blood sample by venipuncture into a citrate-coated container. Approximately 3–5 ml of PRP can be obtained from 30 ml of blood, resulting in an efficiency of around 10% by volume. The first centrifugation of the sample divides the tube into three layers: an upper layer containing mainly plasma and platelets; a middle layer containing leukocytes; and a lower layer containing red blood cells [18]. Whether the final product is leukocyte-rich or -leukocyte-poor determines whether the upper layer is collected with the entire leukocyte layer or only the surface layer.
Aim of the study
This study aims to review and analyze the current literature on the use of PRP as an adjunctive therapy in the treatment of chronic wounds such as pressure ulcers. The review will focus on the therapeutic effects, and potential problems and limitations associated with its use.
Material and methods
A narrative review of the literature on the use of PRP in treating chronic, difficult-to-heal wounds in adults was conducted. The literature search covered publications from 2020 to 2025 in the PubMed and Scopus databases. The search strategy included the following key words and combinations thereof: “platelet-rich plasma,” “PRP,” “chronic wounds,” “pressure ulcer,” and “pressure injury.”
The review included randomized controlled trials on the topical or injectable use of PRP. Systematic reviews, meta-analyses, trial protocols, case reports, and publications not available in English were excluded from the analysis.
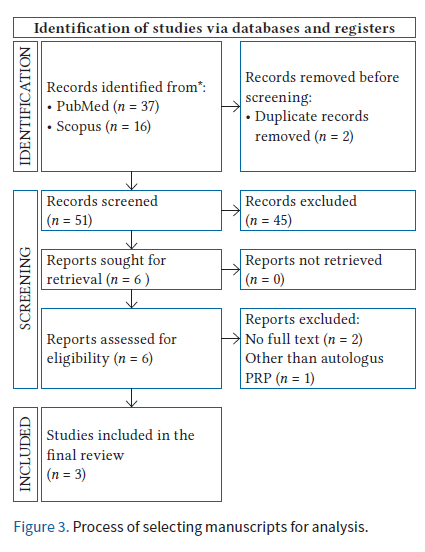
A total of 53 manuscripts were reviewed (37 from PubMed and 16 from Scopus), two of which were duplicates. Fifty-one manuscripts were eligible for analysis. Of these, 45 were rejected based on the titles and abstracts because they did not meet the review criteria. In accordance with the established methodological criteria, additional publications were excluded from the review due to a lack of full text or focus on wounds other than chronic wounds. This resulted in a final analysis of three studies involving adult patients undergoing pressure ulcer treatment (Fig. 3).
Results
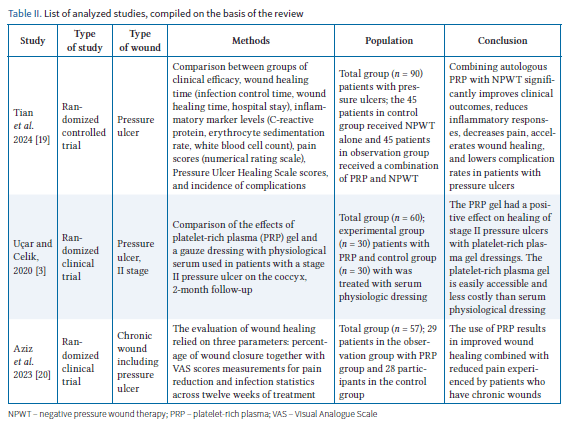
Three studies evaluating PRP in pressure ulcer wounds were included in the analysis. A total of 207 patients with pressure ulcers were examined (Table II). Analysis of the available literature showed that all three of the included studies indicated a faster reduction in wound area, decreased exudate, and shorter treatment and healing times compared to standard dressings [3, 19, 20]. In the study group of patients who underwent PRP and NPWT therapy, the times for infection control, wound healing, and hospital stay were significantly shorter compared to the control group [19].
Platelet-rich plasma therapy reduces levels of inflammatory factors, such as C-reactive protein, erythrocyte sedimentation rate, and white blood cells, and reduces pain [19].
Shortening the healing time has also been shown to reduce the cost of treating pressure ulcer patients [3].
Furthermore, no side effects, such as allergic reactions, have been shown in studies [3, 19, 20].
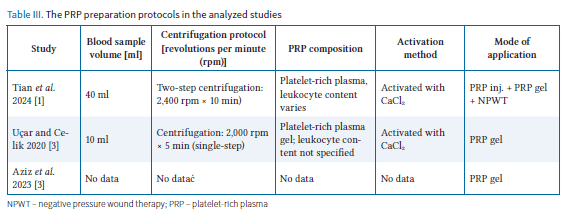
One limitation of PRP therapy for chronic wound healing is the lack of standardization in PRP product collection. PRP preparation protocols in clinical trials are inconsistent, and the analyzed studies do not describe the necessary methods for reproducibility of the protocol. The PRP preparation procedure was also analyzed (Table III).]
Discussion
This review suggests that PRP therapy may support the wound healing process in adults with chronic venous ulcers, diabetic ulcers, and pressure ulcers when healing is delayed or stalled. The therapy is safe and painless, and the fact that it is a biological dressing derived from the patient themselves makes it easily accessible. The healing process may stop due to infection, tissue ischemia, comorbidities such as diabetes, or an absence of proper treatment. Nevertheless, studies have shown that PRP therapy stimulates the wound healing process and reduces wound size, thereby shortening the healing time [3, 19, 20].
Clinical studies demonstrate that PRP can stimulate granulation tissue formation, reduce wound size, decrease exudate, and shorten healing time in patients with pressure ulcers. Uçar and Çelik demonstrated that PRP gel significantly reduced ulcer area and exudate compared with saline gauze dressings at both the initial assessment and after two months. Additionally, total treatment costs were lower in the PRP group [3].
The ability of PRP to accelerate pressure ulcer healing was also confirmed by Tian et al. [19], who compared PRP therapy with negative pressure wound therapy (NPWT) in patients with chronic pressure ulcers. Negative pressure wound therapy improves local blood circulation, accelerating granulation tissue proliferation and reducing tissue edema [21]. In a study of 90 patients with non-healing pressure ulcers lasting eight weeks, the mean healing time was significantly shorter in the PRP group compared with the NPWT group: 29.13 ±2.34 days versus 38.27 ±2.65 days, respectively. Overall treatment efficacy was 95.56% in the PRP group versus 80% in the control group [19].
Similar results were observed by Yang et al. [21] in a study of 84 patients with pressure ulcers. The group receiving combined PRP and NPWT achieved the best outcomes and shortest healing times. Additionally, patients in this group reported lower pain levels than those in the monotherapy groups. To further validate the efficacy of the treatment, the study group underwent computed tomography (CT) imaging. Convolutional neural networks (CNNs) were then used to reduce image noise, which allowed for more precise visualization of wound depth, accurate diagnosis, and appropriate treatment [21].
Studies also demonstrate the satisfactory results of PRP in treating of diabetic foot ulcers when combined with other methods such as NPWT, PRP combined with hyaluronic acid, or adipose-derived stem cells [22–24]. Nolan et al. [23] showed that PRP serves as an effective carrier for adipose-derived stem cells, which can enhance graft survival primarily through early angiogenesis, leading to faster graft revascularization. The researchers conducted this study on 18 patients with diabetic foot ulcers. Histological examination one week after the administration of fat grafts with PRP demonstrated an increase in vascular density. This innovative therapy may accelerate wound healing in diabetic foot ulcers at both the histological and clinical levels, but further studies are needed.
The prolonged hospitalization time associated with the lengthy healing processes increase the cost of treating patients with wounds. In their study on the impact of PRP on reducing healing time, Uçar and Çelik [3] analyzed the costs of associated with the entire healing process. They showed that the total cost, including the purchase of a centrifuge, is one-third lower than that of standard treatment. It should be noted that the purchase of a centrifuge is a one-time expense that will significantly reduces subsequent treatment costs when this method is used.
Multiple clinical studies have demonstrated the effectiveness of PRP in the healing of diabetic foot ulcers [24, 25]. Ullah et al. [26] reported that in a study of 160 patients (80 in the PRP group and 80 in the control group), PRP treatment significantly improved healing outcomes compared to the control group. During follow-up, PRP therapy was associated with a decreased in HbA1c levels, and faster wound healing in patients with a normal BMI [26]. Alamdari et al. [27] found that the mean healing time for diabetic foot ulcers treated with PRP was 68.1 ±16.6 days. Regardless of age, hypertension, or smoking status, healing time was reduced, though PRP did not reduce the risk of amputation [27].
Platelet-rich plasma also has a beneficial effect on accelerating the healing of venous ulcers when combined with compression therapy; however, it does not prevent recurrence after wound closure, as demonstrated in a one-year follow-up study by Elbarbary et al. [15]. From a clinical perspective, PRP can be a valuable adjunct in the comprehensive management of chronic wounds, provided that underlying causative factors – such as prolonged pressure, immobility, chronic venous insufficiency, or neuropathy – are also addressed simultaneously.
As already mentioned there are no clear regulations regarding the formulation and composition of injectable PRP, which may vary in terms of platelet and white blood cell content, red blood cell contamination, and PGF concentrations. The choice of PRP activation method can affect its physical form and the release of growth factors [5]. Therefore, further research is needed to establish a consensus on PRP-related bioformulation terminology, ensuring adequate and safe treatment of specific pathologies and conditions [17, 28].
The choice of treatment method (local application or injection of PRP), contamination of the PRP with microorganisms during the blood collection, manufacturing and administration processes, removal of the PRP gel during the surgical debridement of the ulcer and patient-related factors (including a higher BMI, uncontrolled diabetes, anemia, smoking, kidney problems with a lower glomerular filtration rate, thrombosis, a huge wound, the presence of scar tissue in the wound, infections and nutritional deficiencies) may all affect the effectiveness of PRP. In the case of diabetes, the effectiveness of PRP may be reduced by low platelet counts and decreased cell activity [29].
Another potential issue when obtaining PRP is the patient’s use of non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, naproxen, and diclofenac, as these have antiplatelet effects [29]. The NSAIDs inhibit platelet aggregation by antagonising cyclooxygenase (COX) 1 and 2 and reducing the release of growth factors, which may reduce the therapeutic effect of PRP [29]. In this case, NSAIDs should be discontinued before the planned PRP treatment. Naproxen requires a discontinuation period of 24–48 hours, whereas ibuprofen and diclofenac no longer inhibit platelet aggregation after 6–12 hours, depending on the dose [29].
Similarly, anticoagulants and antiplatelet drugs are commonly used in patients eligible for PRP. As they affect platelet stability, anticoagulants influence the effectiveness of PRP and must be discontinued well before injection therapy [30]. Understanding the pharmacokinetics and effects on platelets can help determine the most appropriate time to stop and then restart a particular anticoagulant. One example is aspirin, which affects platelet viability for up to 10 days.
It is difficult to conduct a reliable analysis of the impact of PRP therapy on improving the healing of pressure ulcer, if only because of the lack of a clear procedure for preparing the preparation. Variables related to the patient’s multimorbidity and the medications taken, which may affect the quality of the preparation obtained, must also be taken into account. However, the studies analyzed show the potential of PRP in the treatment of chronic wounds, including pressure ulcers.
Conclusions
A review of the literature indicates that preparing and using PRP is a safe and straightforward procedure for treating local pressure ulcers. Using PRP is associated with faster reduction of the wound surface area, reduction of exudate, reduction of inflammation and pain, and shorter total treatment time compared to standard dressings.
Platelet-rich plasma can be effectively combined with other therapies or dressings. Using PRP with NPWT increases the effectiveness of the therapy, significantly reducing the time needed for infection control, wound healing, and length of hospitalization compared to conventional treatment. Consequently, it can reduce treatment costs.
Platelet-rich plasma is a safe method; no adverse effects, including allergic reactions, were reported in the analyzed studies.
One limitation is the lack of standardization of the procedure. Differences in PRP preparation methods and insufficient descriptions of protocols in studies limit the ability to reproduce results and compare studies.
Platelet-rich plasma is a promising, effective, and safe method for treating pressure ulcers. However, uniform, standardized protocols must be developed for PRP preparation and use to increase the reliability and comparability of future studies.
Efforts should be made to facilitate access to autologous therapies in clinical practice to enhance opportunities for future research and clinical observation.
Disclosures
The authors declare no conflict of interest.
The study was funded by a grant from the Ministerstwo Edukacji i Nauki in Poland as part of the Progres_Nurs project, conducted under the “Social Responsibility of Science” grant SONP/SP/548059/2022.
Approval of the Bioethics Committee was not required.
References
- Guo SC, Tao SC, Yin WJ, et al. Exosomes derived from platelet-rich plasma promote the re-epithelization of chronic cutaneous wounds via activation of YAP in a diabetic rat model. Theranostics 2017; 7: 81–96. DOI: 10.7150/thno.16803.
- Martinez-Zapata MJ, Martí‐Carvajal AJ, Solà I, et al. Autologous platelet‐rich plasma for treating chronic wounds. Cochrane Database Syst Rev 2016; 2016: CD006899. DOI: 10.1002/14651858.CD006899.pub3.
- Uçar Ö, Celik S. Comparison of platelet‐rich plasma gel in the care of the pressure ulcers with the dressing with serum physiology in terms of healing process and dressing costs. Int Wound J 2020; 17: 831–841. DOI: 10.1111/iwj.13344.
- Jawień A, Grzela T, Ochwat A. Prevalence of chronic venous insufficiency (CVI) in men and women of Poland. Multicenter cross-sectional study of 40095 patients. Phlebology 2003; 18: 110–122.
- Zanzov E, Anastasova V, Ivanova K, Kiskinov P. Platelet-Rich Plasma for Wound Healing in Diabetic Patients. Medicina (Kaunas) 2025; 61: 1535. DOI: 10.3390/medicina61091535.
- Hu Z, Xv H, Feng A, et al. Efficacy and Safety of Platelet-Rich Plasma for Pressure Ulcers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int J Low Extrem Wounds 2024; 18: 15347346241227001. DOI: 10.1177/15347346241227001.
- National Pressure Ulcer Advisory Panel (NPUAP). NEW 2014 prevention and treatment of pressure ulcers: clinical practice guideline. Available at: http://www.npuap.org/resources/educationaland-clinical-resources/prevention-and-treatment-of-pressure-ulcers-clinical-practice-guideline (Access: 12.11.2025).
- Kunder V, Sharma KC, Rizvi Z, et al. The Use of Platelet-Rich Plasma in the Treatment of Diabetic Foot Ulcers: A Scoping Review. Cureus 2023; 15: e43452. DOI: 10.7759/cureus.43452.
- Liu X, Li X, Wei W, et al. Local autologous platelet rich plasma injection combined with platelet rich fibrin filling as the main treatment for refractory wounds: A case series. Front Surg 2023; 9: 1003691.DOI: 10.3389/fsurg.2022.1003691.
- Eppley BL, Woodell JE, Higgins J. Platelet quantification and growth factor analysis from platelet-rich plasma: Implications for wound healing. Plast. Reconstr Surg 2004; 114: 1502–1508. DOI: 10.1097/01.PRS.0000138251.07040.51.
- OuYang H, Tang Y, Yang F, et al. Platelet-rich plasma for the treatment of diabetic foot ulcer: a systematic review. Front Endocrinol (Lausanne) 2023; 14: 1256081. DOI: 10.3389/fendo.2023.1256081.
- Meznerics FA, Fehérvári P, Dembrovszky F, et al. Platelet-Rich Plasma in Chronic Wound Management: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J Clin Med 2022; 11: 7532. DOI: 10.3390/jcm11247532.
- Suthar M, Gupta S, Bukhari S, Ponemone V. Treatment of chronic non-healing ulcers using autologous platelet rich plasma: a case series. J Biomed Sci 2017; 24: 16. DOI: 10.1186/s12929-017-0324-1.
- Ahmed M, Reffat SA, Hassan A, Eskander F. Platelet-Rich Plasma for the Treatment of Clean Diabetic Foot Ulcers. Ann Vasc Surg 2017; 38: 206–211. DOI: 10.1016/j.avsg.2016.04.023.
- Elbarbary AH, Hassan HA, Elbendak EA. Autologous platelet‐rich plasma injection enhances healing of chronic venous leg ulcer: A prospective randomised study. Int Wound J 2020; 17: 992–1001. DOI: 10.1111/iwj.13361.
- Shao S, Pan R, Chen Y. Autologous Platelet-Rich Plasma for Diabetic Foot Ulcer. Trends Endocrinol Metab 2020; 31: 885–890. DOI: 10.1016/j.tem.2020.10.003.
- Everts P, Onishi K, Jayaram P, et al. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int J Mol Sci 2020; 21: 7794. DOI: 10.3390/ijms21207794.
- Akbarzadeh S, McKenzie MB, Rahman MM, Cleland H. Allogeneic Platelet-Rich Plasma: Is It Safe and Effective for Wound Repair? Eur Surg Res 2021; 62: 1–9. DOI: 10.1159/000514223.
- Tian B, Yang X, Liu Y, et al. The application effect of autologous platelet-rich plasma combined with negative pressure sealing drainage technology in pressure ulcer wound repair. Medicine (Baltimore) 2024; 103: e39672. DOI: 10.1097/MD.0000000000039672.
- Aziz AM, Nabi HU, Malik E, Perveen Z, Zafar K, Kashif M. Role of autologous platelet rich plasma in management of chronic wounds. Front Health Inform 2023; 12: 2676–7104.
- Yang J, Xiao C, Wen H, et al. Effect Evaluation of Platelet-Rich Plasma Combined with Vacuum Sealing Drainage on Serum Inflammatory Factors in Patients with Pressure Ulcer by Intelligent Algorithm-Based CT Image. Comput Math Methods Med 2022; 2022: 8916076. DOI: 10.1155/2022/8916076.
- Kartika RW, Alwi I, Suyatna FD, et al. Wound Healing in Diabetic Foot Ulcer Patients Using Combined Use of Platelet Rich Fibrin and Hyaluronic Acid, Platelet Rich Fibrin and Placebo: An Open Label, Randomized Controlled Trial. Acta Med Indones 2021; 53: 268–275.
- Nolan GS, Smith OJ, Heavey S, et al. Histological analysis of fat grafting with platelet‐rich plasma for diabetic foot ulcers – A randomised controlled trial. Int Wound J 2021; 19: 389–398. DOI: 10.1111/iwj.13640.
- Wang Y, Liu B, Piet Y, et al. Risk factors for diabetic foot ulcers mortality and novel negative pressure combined with platelet-rich plasma therapy in the treatment of diabetic foot ulcers. Front Pharmacol 2022; 13: 1051299. DOI: 10.3389/fphar.2022.1051299.
- Li L, Chen D, Wang Ch, et al. Autologous platelet-rich gel for treatment of diabetic chronic refractory cutaneous ulcers: A prospective, randomized clinical trial. Wound Repair Regen 2015; 23: 495–505. DOI: 10.1111/wrr.12294.
- Ullah A, Jawaid SI, Pir Naveed Ahmed Ahsan Qureshi, et al. Effectiveness of Injected Platelet-Rich Plasma in the Treatment of Diabetic Foot Ulcer Disease. Cureus 2022; 14: e28292. DOI: 10.7759/cureus.28292.
- Alamdari NM, Shafiee A, Mirmohseni A, Besharat S. Evaluation of the efficacy of platelet-rich plasma on healing of clean diabetic foot ulcers: A randomized clinical trial in Tehran, Iran. Diabetes Metab Syndr 2021; 15: 621–626. DOI: 10.1016/j.dsx.2021.03.005.
- Elgarhy LH, El-Ashmawy AA, Bedeer AE, Al-Bahnasy AM. Evaluation of safety and efficacy of autologous topical platelet gel vs platelet rich plasma injection in the treatment of venous leg ulcers: A randomized case control study. Dermatol Ther 2020; 33: e13897. DOI: 10.1111/dth.13897.
- Leach T, Huang B, Kramer N, et al. A Review of Platelet-Rich Plasma Use in Patients Taking Non-steroidal Anti-inflammatory Drugs for Guideline Development. Cureus 2024; 16: e71706. DOI: 10.7759/cureus.71706.
- Ramsook RR, Danesh H. Timing of Platelet Rich Plasma Injections During Antithrombotic Therapy. Pain Physician 2016; 19: E1055–E1061.