Original paper | Artykuł oryginalny
The use of the ankle-brachial index in assessing the risk of developing heel pressure ulcers in critically ill patients – preliminary report
Anna Surmacz ![]() 1,2,3, Izabela Sałacińska
1,2,3, Izabela Sałacińska ![]() 2,3, Ewa Kucharska
2,3, Ewa Kucharska ![]() 1, Marek Wasylewicz1, Anna Nowak4, Dariusz Bazaliński
1, Marek Wasylewicz1, Anna Nowak4, Dariusz Bazaliński ![]() 1,2,3
1,2,3
1 Father B. Markiewicz Podkarpackie Oncology Centre, Specialist Hospital in Brzozow, Poland
2 Institute of Nursing, Faculty of Health Sciences and Psychology, Collegium Medicum, University of Rzeszow, Poland
3 Laboratory for Innovative Research in Nursing, University Center for Research and Development in Health Sciences Faculty of Health Sciences and Psychology, Collegium Medicum, University of Rzeszow, Poland
4 School of Foreign Languages, University of Rzeszow, Poland
Address for correspondence:
Anna Surmacz, Institute of Nursing, Faculty of Health Sciences and Psychology, Collegium Medicum, University of Rzeszow, 35-959 Rzeszow, Poland, e-mail: annwojcik@ur.edu.pl
Received: 27.11.2025; Accepted: 19.01.2026
LECZENIE RAN 2025; 22 (4): 135–144
DOI: https://doi.org/10.60075/lr.v22i4.122![]() Artykuł (PDF)
Artykuł (PDF)
Table of contents:
Abstract
Introduction
Material and methods
Results
Discussion
Conclusions
Disclosures
References
Abstract
Introduction: The incidence of pressure ulcers on the heels of critically ill patients is a common, multifactorial phenomenon related to their general condition, the quality of their peripheral perfusion, friction forces, static and shear pressure, immobilisation and specific pharmacotherapy. The aim of this study is to use the ankle-brachial index to assess the risk of critically ill patients developing ischaemic pressure ulcers.
Material and methods: A prospective observational study involving controlled observation and estimation was conducted on a group of 120 patients. A comprehensive literature review was conducted to determine the prevalence of pressure ulcer incidence among critically ill patients. A three-part scientific research protocol was developed. The risk of pressure ulcers was assessed by measuring the ankle-brachial index and using the Braden questionnaire. The skin around the heels was inspected twice.
Results: Infusion of catecholamines has been shown to reduce peripheral perfusion, thereby increasing the risk of pressure ulcer development in critically ill patients (p < 0.001). Reduced distal perfusion, as measured by the ankle-brachial index (ABI), has been shown to be a significant predictor of heel ulcers in critically ill patients (p = 0.026).
Conclusions: Patients hospitalised in the intensive care unit are at particularly high risk of developing pressure ulcers on their heels. Impaired distal perfusion and specific pharmacotherapy have been identified as significant risk factors for pressure ulcer development. The ankle-brachial index is a reliable, cost-effective method of evaluating peripheral circulatory disorders.
Key words: intensive care, pressure ulcers in the heels, critically ill patient, ankle-brachial index.
Introduction
Hospital-acquired pressure ulcers (HAPUs) are an inevitable health problem that can arise during highly specialised medical procedures. Pressure injuries can occur during prolonged surgery and non-specific surgical positioning, as well as during intensive care. Despite preventive procedures, increased risk assessment and regular monitoring being implemented, the risk of pressure ulcers during this period exceeds 15%. Patients undergoing anaesthesia and surgery are predisposed to acute, localised tissue injury associated with pressure, which occurs in the skin and/or underlying soft tissues within 48 to 72 hours [1].
The specific nature of intensive care units means comprehensive prevention is often ineffective due to patients’ serious conditions, multiple organ failure, circulatory failure, pharmacotherapy (anaesthesia, catecholamines) and the effects of physical forces (friction, shearing and static pressure). Patients hospitalised in intensive care units require complex, invasive procedures such as renal replacement therapy or ventilator therapy. In these cases, immobilisation is an important factor in ensuring the effectiveness of the medical procedures. The risk of pressure ulcers developing in critically ill patients is very high, with ulcers in the heel area occurring at a prevalence rate of 18.5–38.9% [2]. The risk of pressure injuries (PI) in the heel area is associated with ischaemic aetiology, resulting not only from its anatomical distance from the heart, but also from impaired distal perfusion depending on comorbidities (e.g. diabetes, peripheral atherosclerosis), general condition (e.g. age, immobilisation, impaired consciousness) and pharmacotherapy. In terms of prevention, the distal parts of the limbs, such as the fingers, ankles and heels, are particularly vulnerable due to inevitable tissue perfusion disorders and coexisting atherosclerosis in people over 60 years of age. The heel has a unique structure consisting of a small amount of subcutaneous tissue, and close contact between bone and tendon structures may pose an infection risk to these structures. The presence of medical devices such as splints and stabilisers is an additional risk factor, as these may increase pressure and lead to pressure ulcers. Pressure ulcer risk is significantly higher in critically ill patients than in conservative or surgical wards. Impaired distal perfusion resulting from primary atherosclerosis and subsequent vasoconstriction caused by catecholamine action may lead to local oedema, ischaemia, and secondary pressure ulcers. An additional factor related to tissue oxygenation is mechanical ventilation, as well as blood pH (acidosis/alkalosis) and its effect on blood oxygenation, which in turn can affect inefficient cellular processes and, consequently, cell death. Since 2009, there have been reports of a correlation between the risk of developing pressure ulcers and the occurrence of metabolic disorders and an increase in serum pH [3]. However, when analyzing the literature on pressure ulcers in the heel area, the main risk factors mentioned by the authors are often mechanical ventilation and immobilization [3, 4]. Cardiovascular failure can result from disease processes such as shock decompensation and hypotension, which, according to the literature, are strong risk factors for local ischemia at the site of pressure. The authors indicate that maintaining a mean arterial pressure (MAP) of 85 mmHg reduces the risk of tissue hypoxia, thereby reducing the risk of hypoxia. The authors indicate that the mean arterial pressure measurement parameter provides a broad picture of tissue perfusion, which is directly related to vasopressor pharmacotherapy. Mean arterial pressure as an indirect parameter indicates the patient’s general condition, the severity of shock, and the need to use catecholamines to achieve adequate perfusion. Regarding to the risk of pressure ulcers, the level of tissue perfusion is an important factor that can influence the development of pressure ulcers, as well as the healing process [5]. However, the standard procedure is to administer catecholamines, which constrict blood vessels, thereby reducing peripheral perfusion. Furthermore, immobilisation and loss of lean muscle mass may increase the risk of pressure ulcers in this group of patients. Despite the implementation of preventive measures such as repositioning, the use of aids, and anti-pressure ulcer mattresses, patients in severe, critical condition may develop pressure ulcers during hospitalisation. The risk of developing pressure ulcers is high and they occur independently. Clinical observations indicate that pressure ulcers develop during hospitalisation in situations of malnutrition, immobilisation and the implementation of intensive care unit-typical pharmacotherapy. The development of pressure ulcers on the heels of critically ill patients is caused by early changes in the arteries, which can be identified by performing an ankle-brachial index (ABI) test. Distal perfusion disorders are a serious problem that is often underestimated. Neubauer-Geryk and Bieniaszewski [6] discuss the problem of atherosclerosis and points out that the course of the disease itself is often asymptomatic. A cheap and simple method of early identification of ischemia is to assess the lower limb arteries using the ABI [7]. The risk of atherosclerosis is particularly high in patients with a history of diabetes, as highlighted in the paper on ABI in a group of patients with vascular ulcers by Cwajda and Białasik [8]. There is an increasing amount of literature on the validity of assessing distal perfusion using the ABI. In 2017, recommendations for wound treatment that emphasised the need to use the ABI as a routine check of distal blood flow were developed in Italy [9].
The aim of this study was to assess the risk of developing ischemic pressure ulcers in a group of critically ill patients using the ABI.
Material and methods
This prospective observational study used a controlled observation and estimation method. Short-term controlled observation was performed on 120 patients (54 women and 66 men), with a mean age of 67 years. The study period was 18 months. All patients underwent prevention based on Polish Wound Management Association 2020 recommendations, which included body position changes, high-profile tubular mattresses and pressure-relieving skincare. The study was conducted at Fr. B. Markiewicz Specialist Hospital of the Podkarpackie Oncology Centre in Brzozow. Consent from the head of the department and the director of the facility was obtained. The study was conducted in two stages. The first stage took place within 24 hours of admission, and the second stage on the 5th–10th day of hospitalization in the ward. Because a basic requirement of the study is the participation of critically ill, unconscious, mechanically ventilated patients, it was impossible to obtain the patient’s informed consent at the time of inclusion in the study. The patient’s consent or objection was obtained at the time of regaining consciousness. In the case of critically ill patients, consent was obtained from a legal representative. In the event of death, the patient was excluded from the study.
A literature review was conducted on the subject, incorporating the National Pressure Injury Advisory Panel (NPIAP)/European Pressure Ulcer Advisory Panel (EPUAP) (2019) and Polish Wound Management Association (2020) recommendations. Based on the literature, a scientific and research protocol was developed. The first part contained information on socio-demographic data, chronic diseases, reasons for admission and patient categorisation in the intensive care unit (ICU), based on the 2016 Regulation of the Minister of Health [10, 11]. Measurement results include the ABI and Braden scale. The second part contains a questionnaire for assessing skin damage on the heels according to the NPIAP classification. The study was conducted in two stages. During the study, the ABI was assessed using a MESI mTABLET device with ISO 9007 Q-1664 specifications and a CE 1304 ISO 9001/ISO 13485 certificate. The examination was conducted by a medically qualified professional experienced in assessing patients’ conditions using the indicated method. In cases of non-diagnostic peripheral artery disease (PAD), if critical ischaemia was confirmed, a surgical consultation involving a duplex ultrasound scan was performed. During the study’s planning stage, the inclusion criteria were defined as follows: age over 18 years; inability to self-care due to sedation; respiratory failure requiring ventilator therapy; respiratory support (continuous positive airway pressure [CPAP] or noninvasive ventilation [NIV]); infusion of catecholamines; shock; haemodynamic failure; and condition after cardiac arrest. The following exclusion criteria were adopted: lack of consent from the patient/authorised person to participate in the study; stable general condition without the need for mechanical ventilation; and admission of patients to the ICU with respiratory failure after surgery, who were planned to be discharged after the cessation of neuromuscular blockade, provided that the patient exhibited spontaneous and efficient breathing.
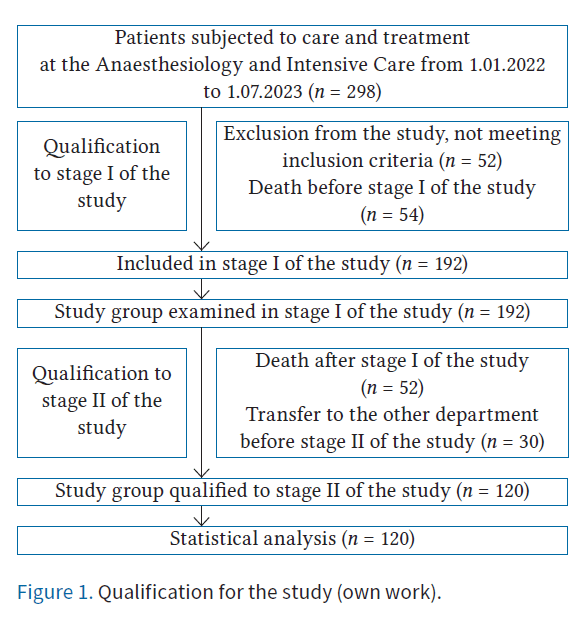
The qualification of the study group is presented in Figure 1.
Characteristics of the study group
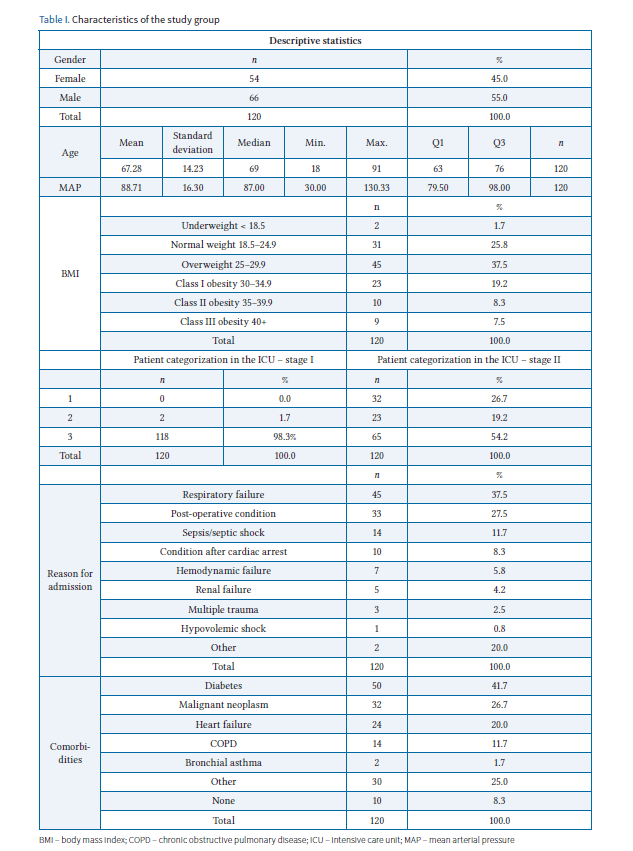
The study group consisted of 120 patients hospitalised in the anaesthesiology and intensive care unit, including 54 women (45%) and 66 men (55%). The mean age of the subjects was 67 years, with a mean deviation of 14.23 and a median of 69 years. In the body mass index (BMI) assessment, normal values were recorded in 25.8% (n = 31) of patients, underweight values in 1.7% (n = 2), class I obesity in 19.2% (n = 23), class II obesity in 8.9% (n = 10) and class III obesity in 7.5% (n = 9) of patients. In the first stage of the study, patient classification score in the ICU was assessed. It was noted that 98.5% of subjects (n = 118) in terms of care were category III and 1.7% (n = 2) were category II. In the second stage, category I care was observed in 26.7% of patients (n = 32), category II in 19.2% (n = 23) and category III in 54.2% (n = 65). The most common reasons for ICU admission were respiratory failure (37.5%, n = 45), postoperative condition (27.3%, n = 33) and sepsis/septic shock (11.7%, n = 14). The most prevalent chronic diseases identified through medical record analysis were diabetes (14.7%, n = 50), malignant neoplasms (36.7%, n = 32), and heart failure (20%, n = 24). In the first stage of the study, MAP values were assessed, with an average value of 88.71 mmHg. Detailed data are presented in Table I.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics version 21. Descriptive statistics, histograms, box plots, scatter plots and Kolmogorov–Smirnov normality tests were employed to evaluate the variables. Analytical techniques used to analyse relationships between variables and verify research hypotheses included the following: Spearman’s rank correlation coefficient; Kruskal–Wallis and Mann–Whitney U tests to analyse differences in the distribution of dependent variables in relation to independent variables; and χ2 tests to analyse the independence of variables in contingency tables. Regarding the assumptions of the planned power analysis (α = 0.05, power = 0.80, medium effect size), the sample size was sufficient for precise determination of the mean ABI (n required ≈ 35). For correlation analyses with a value of r = 0.3 (n required ≈ 84). The power analysis indicates that there is a small risk of not detecting a medium-sized effect in the analyses of differences between groups, while the sample size was sufficient or greater than required for the other analyses.
Bioethical standards
The study was approved by the Bioethics Committee at the University of Rzeszow (approval No. 2022/064).
Results
Treatment administered
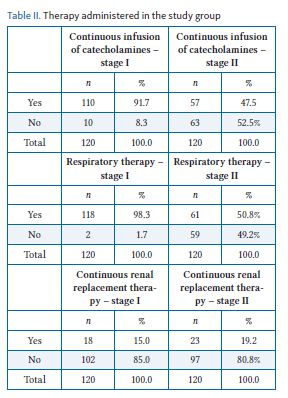
The entire study group required multidisciplinary treatment due to life-threatening conditions of various aetiologies (Table II). In stage I of the study, a continuous infusion of catecholamines was administered to 97.7% (n = 110) of participants, whereas in stage II, this was required by only 47.5% (n = 57) of participants. Noradrenaline was the most commonly used infusion (in 86.6% of participants, n = 104), followed by dobutamine (10.0%, n = 12). Mechanical ventilation was required by 98.3% (n = 118) of patients in stage I of the study and by 50.8% (n = 61) in stage II. Continuous renal replacement therapy was required by 15.0% (n = 18) of patients in stage I and 19.2% (n = 23) in stage II.
Ankle-brachial index
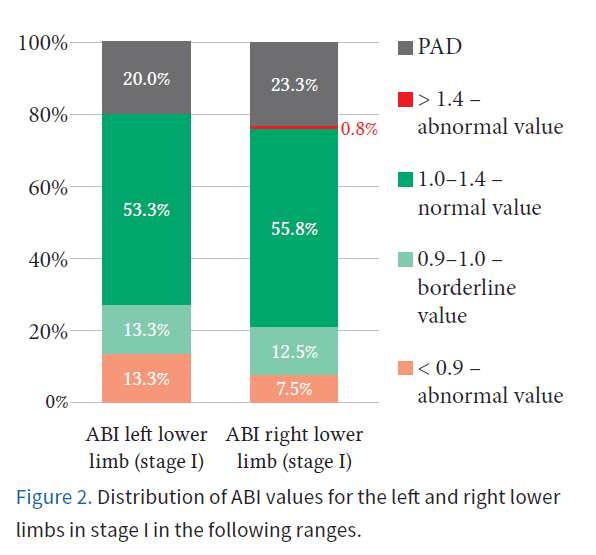
During stage I of the study, the ABI was assessed. The average ABI value was 1.08 for the left limb and 1.11 for the right limb. Normal ABI values were observed in 53.3% of subjects in the left lower limb and in 55.8% in the right lower limb. Non-diagnostic PAD values were found in 20% of subjects for the left lower limb and in 23.3% for the right lower limb. Borderline values were found in 13.3% of subjects for the left lower limb and 12.5% for the right. Abnormal values were found in 13.3% of patients for the left lower limb and in 7.5% for the right lower limb. Figure 2 shows the distribution of ABI values for the left and right lower limbs.
Risk of pressure ulcers according to the Braden assessment
During the study, the risk of pressure ulcer development was assessed using the Braden Scale in Stage I. This revealed a very high risk in 59.2% of subjects and a high risk in 36.7%. Stage II showed a downward trend, with very high risk reported in 27.5% of patients, high risk in 42.5%, and moderate risk in 10%. These results suggest a slight reduction in the risk of pressure ulcers in stage II of the study (Table III).
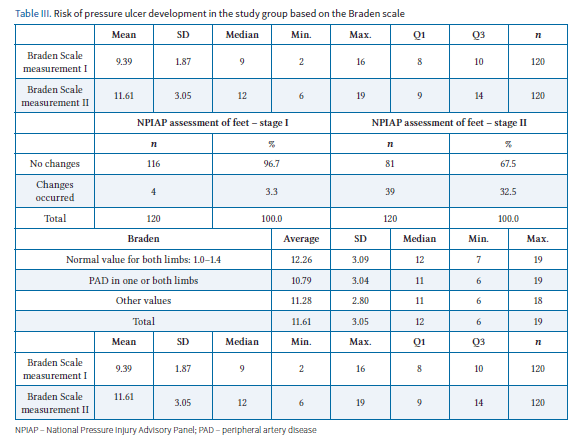
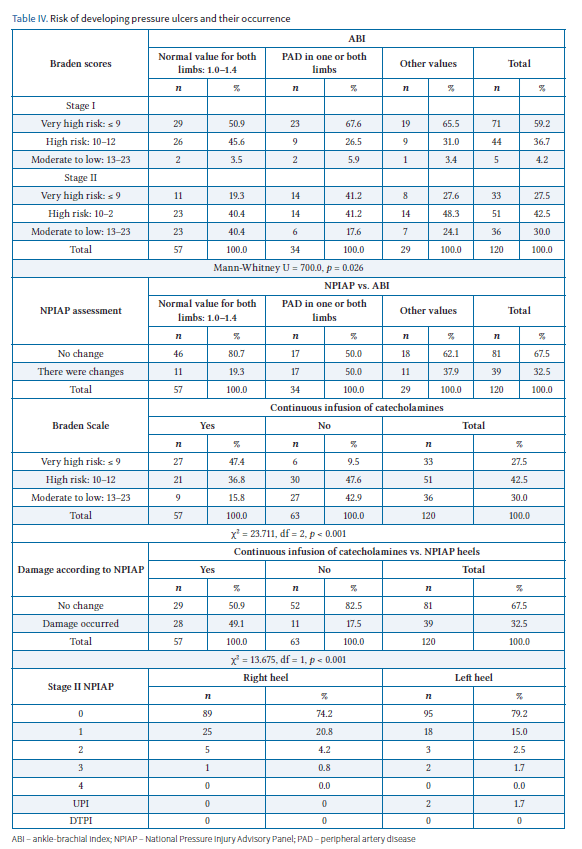
During the study, the skin on the heels was examined and stage 1 pressure ulcers were found on the right heel in 20.8% (n = 25) of subjects and on the left heel in 15% (n = 18). Stage 2 pressure ulcers were found in 4.2% (n = 5) of subjects on the right heel and in 2.5% (n = 3) of subjects on the left heel. Stage 3 pressure ulcers occurred on the right heel in 0.8% (n = 1) of subjects and on the left heel in 1.7% (n = 2). An unspecified UPI pressure ulcer was observed in 1.7% of the subjects. Analysis of the results showed that patients with low ABI values in one or both limbs (i.e. those at risk of peripheral arterial disease) were particularly at risk of developing pressure ulcers on the heels (p < 0.05). A statistically significant correlation was found between the risk of developing pressure ulcers on the heels in patients with PAD (Mann–Whitney U = 700.0, p = 0.026). Pressure ulcers were observed to occur more frequently in patients with PAD than in patients with normal ABI results (p < 0.05).
This finding highlights the significant association between PAD and an increased likelihood of developing pressure ulcers, underscoring the importance of meticulous risk assessment and targeted preventive strategies in this patient group. The subsequent analysis using the Braden Scale provided further insight into the specific risk factors contributing to pressure ulcer development among the study population.
The study showed that patients who received a continuous infusion of catecholamines were more likely to be in the high-risk group for pressure ulcers than those who did not (p < 0.001). Detailed data are presented in Table IV.
Discussion
Patients in intensive care units are at high risk of developing pressure ulcers in areas affected by physical forces, such as the sacrum, trochanter and heels. Despite the known aetiology and risk factors, the problem continues to arise during hospitalisation. In specialist terminology, pressure ulcers that occur during hospitalisation are referred to as HAPI (hospital-acquired pressure injuries). The term “unavoidable pressure ulcers” was introduced in a global consensus in 2014 [12].
Pressure ulcers that develop during hospitalisation are mainly associated with prolonged medical procedures. Patients undergoing long-term treatment, in critical condition or at the end of life are most at risk. Pittman et al. [13] conducted retrospective studies to assess the frequency of possible and unavoidable HAPIs in critically ill patients hospitalised in intensive care units. The authors showed that, of the pressure injuries identified, 60% were preventable and 41% were considered unavoidable. Most of the injuries were described as deep tissue destruction [13].
In the course of our research, which was conducted in the anaesthesiology and intensive care unit, 120 patients were observed, including 54 women (45%) and 66 men (55%). The subjects’ mean age was 67 ±14.23 years, with a median age of 69 years. The most common reasons for ICU admission were respiratory failure (37.5%, n = 45), postoperative condition (27.3%, n = 33) and septic shock (11.7%, n = 14). The most common comorbidities were diabetes mellitus (14.7%, n = 50), malignant neoplasm (36.7%, n = 32) and heart failure (20%, n = 24). Despite implementing pressure ulcer prevention measures based on the Polish Wound Management Association 2020 recommendations [17], HAPI was observed in the heels of 23.14% of subjects. Researchers seeking answers to the question of why pressure ulcers develop during hospitalisation explain their development by skin failure associated with perfusion disorders in critically ill patients [1, 2, 9].
The intensive care unit is a unique place where pressure ulcers in patients occur frequently. This is due to factors related to severe clinical conditions, immobilisation, frequent malnutrition and the need to implement specialised life-saving procedures. Although the PTLR recommendations indicate the tools available in Poland, there is still no specific, dedicated tool for risk assessment in the intensive care unit. This is despite the fact that several questionnaires are available. The intensive care unit is a place with a specific patient profile where risk factors are difficult or impossible to eliminate. Recently, researchers have shown an increased interest in the risk and occurrence of pressure ulcers in intensive care units, with several studies pointing to specific assessment tools that have not yet undergone psychometric evaluation in Poland [15, 16]. These observations suggest ample scope for further scientific research into the evaluation of new risk assessment tools recommended for perioperative prevention. Understanding and quickly identifying risk factors, and implementing preventive protocols, creates opportunities to reduce the risk of pressure ulcers. However, despite the implementation of preventive measures, pressure injuries often occur, not as a result of negligence in care or prevention, but due to general clinical factors. Patient assessment should be carried out according to protocol and based on a physical examination, as well as a skin assessment using the recommended pressure ulcer risk assessment scales. Relying solely on questionnaire-based assessments can lead to potential skin damage being underestimated [15, 17]. Using specialised tools such as thermal imaging cameras or scanners is also recommended [18].
One serious factor that medical personnel initially find very difficult to assess is impaired peripheral perfusion associated with atherosclerosis, the patient’s position, a lack of muscle stimulation and ongoing pharmacotherapy that affects peripheral circulation. Atherosclerosis is asymptomatic in its initial stage, especially in patients with diabetes who do not exhibit the classic symptoms of peripheral artery disease (PAD), and in situations of general deterioration and serious, life-threatening conditions. Catecholamine administration exacerbates this problem, posing a high risk of bedsores, difficult healing processes, and even amputation. The presence of comorbidities, including diabetes, significantly impacts lower ABI values [8]. Using ABI assessment as a screening test, especially in diabetic ICU patients, can effectively contribute to identifying low ABI values as an additional risk factor for pressure ulcer development in the heels and influencing the development of effective pressure ulcer prevention strategies [17, 19].
Our research has confirmed the link between distal perfusion disorders and the risk of pressure ulcers. We observed differences in the incidence of very high-risk bedsores depending on the ABI value. A very high risk of bedsore development was demonstrated, particularly among patients whose ABI assessment in one or two limbs corresponded to PAD (p = 0.026). Pressure ulcers occurred more frequently in the PAD group than in patients with normal results (p = 0.008). Haemodynamic parameters were assessed, including mean arterial pressure (MAP), which averaged 88.71 in the first stage of the study in the study group. Catecholamine infusion was administered to 91.7% of patients in the study group, with an average output of 3.37 ml/h. The most commonly used catecholamines were norepinephrine (86.7%) and dobutamine (10%). A strong correlation was observed between amine treatment and pressure ulcer incidence (p < 0.001). During our research, we observed the actual occurrence of pressure ulcers in the heel area. Grade 1 pressure ulcers according to the NPIAP were confirmed in the right heel in 20.8% of cases (n = 25) and in the left heel in 15% of cases (n = 18). Grade 2 pressure ulcers were found in the right heel in 4.2% of patients (n = 5) and in the left heel in 2.5% of patients. Grade 3 pressure ulcers were present on the right heel of 0.8% (n = 1) of patients and on the left heel of 1.7% (n = 2). These accounted for 40% of the pressure ulcers observed in the study group. The study confirmed a relationship between catecholamine use and pressure ulcer frequency; pressure ulcers occurred more frequently in patients requiring catecholamine infusion than in those not requiring pharmacological circulatory stabilisation (p < 0.001). When the risk of developing pressure ulcers was assessed using the Braden scale in the second stage of the study, a very high risk (47.4%, amounting to 9 points on the Braden scale) was found in patients who received catecholamine infusions. A high risk (36.8%, amounting to 10–12 points) and a moderate risk were also identified. Analysis of the data confirmed a correlation between catecholamine infusion and actual changes to the heels in this patient group (p < 0.001). Further research is needed in several centres using specific assessment scales and scanners or thermal imaging cameras to confirm these observations.
Caring for a patient in an intensive care unit is associated with certain limitations in terms of prevention. These limitations may result from the patient’s critical condition, intolerance to changes in position, rapid deterioration of vital signs and sudden health deterioration. Pressure ulcer prevention should be based on an assessment of the patient’s condition, conducted through physical examination and the use of simple assessment tools, questionnaires and documentation of actions [16]. Side-to-side rotation, heel elevation, skin care, foam dressings and protective footwear, alongside regular skin condition assessments, should be standard procedures to effectively relieve areas particularly vulnerable to simple pressure, friction and shear forces [19–21].
Superficial pressure ulcers are not a clinical problem. Every effort should be made in professional care to prevent deep tissue damage becoming infected. An infected pressure ulcer can have serious consequences for patient care and can create a risk of tendon and bone infection, especially in the foot area, which can lead to sepsis and potential limb amputation.
Conclusions
The development of pressure ulcers on the heels of critically ill patients is the result of many factors and is not due to negligence in care and prevention. The fact that pressure ulcers occur means that the development of wounds is unavoidable. Patients hospitalised in the intensive care unit are particularly at risk of developing pressure ulcers in the heel area. Impaired distal perfusion indicates a high risk of pressure ulcers. Using the ABI is an effective and inexpensive way to screen for peripheral blood flow disorders.
Disclosures
The authors declare no conflict of interest.
This research received no external funding.
The study was approved by the Bioethics Committee at the University of Rzeszow (approval No. 2022/064).
References
- Shang Y, Wang F, Cai Y, et al. The accuracy of the risk assessment scale for pressure ulcers in adult surgical patients: a network meta-analysis. BMC Surg 2025; 25: 104.
- Chaboyer WP, Thalib L, Harbeck EL, et al. Incidence and Prevalence of Pressure Injuries in Adult Intensive Care Patients: A Systematic Review and Meta-Analysis. Crit Care Med 2018; 46: e1074–e1081.
- Senturan L, Karabacak U, Ozdilek S, Alpar SE, Bayrak S, Yüceer S, Yildiz N. The relationship among pressure ulcers, oxygenation, and perfusion in mechanically ventilated patients in an intensive care unit. J Wound Ostomy Continence Nurs 2009; 36: 503–508. DOI: 10.1097/WON.0b013e3181b35e83.
- Pender LR, Frazier SK. The relationship between dermal pressure ulcers, oxygenation and perfusion in mechanically ventilated patients. Intensive Crit Care Nurs 2005; 21: 29–38. DOI: 10.1016/j.iccn.2004.07.005.
- Cox J, Roche S. Vasopressors and development of pressure ulcers in adult critical care patients. Am J Crit Care 2015; 24: 501–510. DOI: 10.4037/ajcc2015123.
- Neubauer-Geryk J, Bieniaszewski L. Ankle-brachial index in the assessment of patients at risk of atherosclerosis. Heart and Vascular Diseases 2007; 4: 1–5.
- Rossa S, Głowacka M, Szewczyk M, Mościcka P, Cwajda-Białasik J, Karpińska A. Wskaźnik kostka–ramię w chorobach naczyń kończyn dolnych. Pielęg Chir Angiol 2018; 12: 85–89.
- Cwajda-Białasik J, Mościcka P, Szewczyk M, Jawień A. Ocena wartości wskaźnika kostka–ramię u chorych z owrzodzeniem kończyny dolnej o etiologii naczyniowej. Pielęg Chir Angiol 2016; 10: 84–91.
- Labeau SO, Afonso E, Benbenishty J, et al.; DecubICUs Study Team; European Society of Intensive Care Medicine (ESICM) Trials Group Collaborators. Prevalence, associated factors and outcomes of pressure injuries in adult intensive care unit patients: the DecubICUs study. Intensive Care Med 2021; 47: 160–169. DOI: 10.1007/s00134-020-06234-9.
- PTAiIT guidelines specifying the rules for qualification and criteria for admission of patients to Anesthesiology and Intensive Care Units; accessed on 14 July 2023.
- Regulation of the Minister of Health of December 12, 2018, amending the regulation on the organizational standard of healthcare in the field of anesthesiology and intensive care (Journal of Laws of 2018, item 2381).
- Edsberg LE, Langemo D, Baharestani MM, Posthauer ME, Goldberg M. Unavoidable pressure injury: state of the science and consensus outcomes. J Wound Ostomy Continence Nurs 2014; 41: 313–334. DOI: 10.1097/WON.0000000000000050.
- Pittman J, Beeson T, Dillon J, Yang Z, Cuddigan J. Hospital-Acquired Pressure Injuries in Critical and Progressive Care: Avoidable Versus Unavoidable. Am J Crit Care 2019; 28: 338–350. DOI: 10.4037/ajcc2019264.
- Chaboyer WP, Thalib L, Harbeck EL, et al. Incidence and Prevalence of Pressure Injuries in Adult Intensive Care Patients: A Systematic Review and Meta-Analysis. Crit Care Med 2018; 46: e1074–e1081. DOI: 10.1097/CCM.0000000000003366.
- Bazaliński D, Szymańska P, Surmacz A, Pytlak K, Barańska B. Psychometric analysis of selected tools for pressure ulcer risk assessment – literature review. Leczenie Ran 2025; 22: 93–103. DOI: https://doi.org/10.60075/lr.v22i3.114.
- Konateke S, Güner Şİ. Development of A Surgery-Related Pressure Injury Risk Assessment Scale (SURPIRAS): A Methodological Study. J Clin Nurs 2025; 34: 4841–4853. DOI: 10.1111/jocn.17765.
- Szewczyk MT, Kózka M, Cierzniakowska K, et al. Pressure ulcer prevention – recommendations of the Polish Wound Management Association. Part I. Leczenie Ran 2020; 17: 113–146.
- Bazaliński D, Pytlak K, Szymańska P, Więch P. The use of thermography in local wound care – two case studies. Leczenie Ran 2023; 20: 77–83. DOI: 10.60075/lrpjwm.v20i2.30.
- Szewczyk M, Cwajda-Białasik J, Mościcka P, et al. Treatment of pressure ulcers – recommendations of the Polish Wound Management Association. Part II. Leczenie Ran 2020; 17: 151–184. DOI: 10.5114/lr.2020.103116.
- Bazaliński D, Szymańska P, Szewczyk M. Odleżyny pięt w świetle wytycznych światowych (EPUAP/NPIAP) i doświadczeń własnych. Przegląd piśmiennictwa. Leczenie Ran 2020; 17: 185–193. DOI: 10.5114/lr.2020.103117.
- Koyanagi M, Sakuramoto H, Kajiwara K, et al. Prophylactic Interventions for Heel Pressure Ulcers in Critically Ill Patients Admitted to an Intensive Care Unit: A Systematic Review and Meta-Analysis. Cureus 2025; 17: e83029. DOI: 10.7759/cureus.83029.
- El Genedy M, Hahnel E, Tomova-Simitchieva T, et al. Cost-effectiveness of multi-layered silicone foam dressings for prevention of sacral and heel pressure ulcers in high-risk intensive care unit patients: An economic analysis of a randomised controlled trial. Int Wound J 2020; 17: 1291–1299. DOI: 10.1111/iwj.13390.