Opis przypadku | Case report
Klingsor syndrome as a rare case of self-amputation of the penis
Piotr Wojda
1 Psychiatric Clinic, Cologne, Germany
Address for correspondence: Psychiatric Clinic, Wilhelm Grisinger Str. 23, Cologne, Germany, e-mail: askot@wp.pl
Received: 25.09.2025 Accepted: 12.11.2025
LECZENIE RAN 2025; 22 (3): 122–126
DOI: https://doi.org/10.60075/lr.v22i3.112
Spis treści:
Abstract
Introduction
Case presentation
Bioethical standards
Discussion
Conclusions
Disclosures
References
Abstract
Genital self-mutilation (GSM) is rare and a serious condition requiring multidisciplinary treatment. Life-saving measures (heavy bleeding) should be initiated first, followed by efforts to restore anatomical continuity and functionality of the damaged structures as much as possible. Concurrently, psychiatric disorders must be treated, wounds appropriately dressed, and support provided to the patient. Total penectomy is associated with long-term deterioration in the patient’s quality of life.
This article presents the case of a patient who self-mutilated his genitals as a result of Klingsor syndrome. The aim of the study is to present the patient’s health problems based on the NANDA nursing diagnoses classification. Patient care should be focused on the patient’s needs, and staff should be provided with current, evidence-based nursing knowledge. A holistic approach to the patient’s problems and the implementation of nursing interventions in accordance with current knowledge prevented complications related to self-harm and positively influenced the improvement of his mental state. Proper wound care is one element of multidimensional care for patients with Klingsor syndrome, but nurses should also recognize other issues arising from the disease.
Key words: Klingsor syndrome, penile self-amputation, wound care, psychiatric nursing.
Introduction
Klingsor syndrome is the deliberate self-mutilation of the genital organs (GSM) in the course of a mental illness, especially psychosis, without suicidal intent [1]. The literature identifies three groups at risk for genital self-mutilation: patients with schizophrenia, transvestites, and men experiencing religious or cultural conflicts [2]. Over 90% of patients who self-mutilated their genital organs had a mental disorder, including 49% with schizophrenia spectrum disorders, substance use disorders such as marijuana or cocaine (19%), personality disorders (16%), gender dysphoria (15%), depression (9%), and bipolar disorder (1%) [1].
The incidence of psychiatric pathologies such as depression, anxiety, and mood disorders is also higher in amputees than in the general population [3]. Self-amputations in those without a psychiatric diagnosis (approximately 9–13%) are attributable to GSM, including sexual conflicts, guilt related to sexual desires, religious beliefs, and unconventional forms of sexual arousal [1,3].
In addition to the risk of infection and anatomical changes, GSM may be associated with an increased risk of suicide, repeated self-harm, and greater severity of psychopathology [1, 3]. It is estimated that 55–85% of people who self-harm attempt suicide [3].
One of problems may be difficulties in caring for wounds after genital amputation. Genital wounds are associated with an increased risk of infection, difficulty maintaining a wound dressing, and pain. Genital wounds heal rapidly, with significant swelling and absent or barely visible scarring, which is related to the anatomical and physiological differences in this region (lack of subcutaneous fat, high mobility of the skin relative to underlying tissues, abundant elastic fibers, persistent bacterial colonization, and rapid resolution of inflammation) [4]. Genital skin defects can be managed using a variety of techniques, including primary closure, local flaps, full-thickness skin grafts, and split-thickness skin grafts [5]. Perineal skin grafting carries the risk of graft rejection due to infection, difficulty in stabilizing the graft due to genital mobility, and fluid accumulation in the form of blood, serous, and purulent exudate. For penile reconstruction (if the amputated portion is inaccessible or not suitable for reimplantation), myoplasty (possible sexual satisfaction) or myocutaneous flap grafting with prosthesis implantation are used [5]. Donor penile transplantation with immunosuppressive therapy is also an option. Another viable treatment option is allogeneic penile transplantation [6].
The aim of the study is to present the patient’s health problems based on the NANDA nursing diagnoses classification. For this purpose, the patient’s condition was assessed, nursing diagnoses were made, nursing interventions were implemented, and their effectiveness was evaluated.
Case presentation
A 40-year-old patient, single, living with his family and unemployed, was admitted from the intensive care unit to a closed psychiatric ward after self-amputation of his penis during cannabinoid-induced psychosis (Fig. 1). The patient underwent urological treatment, which included dressing the injury and inserting a urinary catheter. Penile reconstruction following amputation was not possible. The testicles were preserved. By self-harming his genitals, the patient wanted to prevent a threat to his family from strangers in the home (he heard male and female voices). The patient was hospitalized numerous times for mental disorders caused by psychoactive substances (1 g of marijuana per day), which he had been taking since the age of 16 years. In 2007, the patient, under the influence of drugs, attempted suicide by self-injury to his wrists. Since 2017, the patient has been under the care of a mental health clinic for mood disorders and obsessive-compulsive disorder. The patient currently complains of a depressed mood. He denies auditory hallucinations in the form of voices and distances himself from suicidal intentions. After a psychiatric examination, the diagnosis was: “mental and behavioral disorders caused by marijuana use”.
A physical examination revealed no abnormalities, except being slightly overweight (BMI = 25). Vital signs were normal, skin was pale, anemia was mild, and there were no allergies. Marijuana was detected in the urine. The following medications were taken venlafaxine 225 mg/day, quetiapine 50 mg/day, atorvastatin 10 mg/day, and ibuprofen 600 mg four times daily. Adjunctive treatment included individual psychotherapy, occupational therapy, and consultations with a sexologist.
Initial wound inspection: The amputation wound was oval (2.3 cm × 2 cm) and showed no signs of infection, and the scrotal postoperative wound was 8 cm long with visible surgical sutures, without signs of infection. The amputation wound had minimal exudate, and the wound edges were sunken, with visible surgical sutures securing the skin to the penile stump. The wounds were dressed in adhesive foam dressings, over which the patient wore normal underwear. Medical records from the previous hospitalization did not contain information about wound care or dressings. The patient was assessed for risk of wound infection (WAR scale), pain intensity (Numerical Rating Scale – NRS), nutritional status (Mini Nutritional Assessment – MNA), and willingness to participate in wound care. The patient did not complain of pain during dressing changes.
Wound care: The amputation wound was disinfected with a sterile gauze pad soaked in Octenisept disinfectant and left on the wound for 1 minute. The wound was dressed with a 5 × 7 cm non-adhesive Biatain foam dressing and secured with mesh underwear. This dressing was used for the entire patient’s stay (5 days). Due to the risk of skin trauma, plasters were not used. The dressing was changed daily. The scrotal wound was disinfected with Octenisept and secured with sterile gauze pads. To optimize wound healing, increased caloric, protein, and trace element intake was introduced. After 5 days of stay, the patient was discharged at his request. He received a referral to the wound care outpatient clinic, along with information about his previous wound care and psychiatric outpatient clinic. It is unknown whether the patient complied with these recommendations after discharge.
Bioethical standards
The patient provided informed consent for publication. Institutional ethical review was not required in accordance with local case-control policy (Germany).
Discussion
A patient with a self-inflicted wound required multidisciplinary care. Initially, steps were taken to ensure the patient’s safety and prevent further self-harm or suicide. The next challenge was to create optimal conditions for wound healing by preventing infection, providing appropriate wound care, and meeting the increased nutritional needs. Correctly securing and maintaining the dressing in place posed a challenge. The patient was active, and the anatomical location of the wound made it difficult to fit and adhere the dressing properly. The use of plasters was abandoned due to the risk of damaging the sensitive skin. The use of elastic mesh underwear, which conformed to the body’s shape and stabilized the dressing, resolved this issue. The patient cooperated readily during dressing changes and adhered to wound care and hygiene recommendations. After the injury, the patient experienced psychosocial difficulties, manifesting as concerns about conforming to the cultural image of a man. This required the implementation of long-term individual therapy, sexological counseling, and rehabilitation, as well as tact and sensitivity in daily interactions. The patient refused some of the therapies offered to him (mirror therapy). He found relaxation therapy particularly helpful. Psychiatric treatment was also initiated with continued care in specialized outpatient clinics, depending on the specific problem.
Penectomy-related complications reach 19.7%, with wound infections accounting for 3% and urinary tract infections (UTIs) 3% [13]. Wound infections, malnutrition, and failure to meet the increased demand for energy, macronutrients, micronutrients, and vitamins can lead to an increased risk of wound infection and delayed healing [14, 15]. Nursing interventions implemented in this case effectively prevented the development of a wound infection and supported the healing process.
The patient was catheterized for a long time to divert urine and reduce the risk of wound infection. Conversely, bladder catheterization carries a higher risk of urinary tract infections. It is estimated that 20% of urinary tract obstructions are catheter-related [16]. Compliance with recommendations and patient education regarding catheter-related self-harm did not lead to urinary tract infections. Patients who self-harm are at increased risk of suicide. Evidence demonstrating the effectiveness of structured risk assessment, safety planning, and therapeutic communication underscores the crucial role of nursing in suicide prevention [17].
The loss of his penis through self-amputation impacted his psychological well-being and necessitated a redefinition of his male identity in a hegemonic culture. He feared he would not live up to the socially imposed male role and would not satisfy his sexual needs. The penis is culturally perceived as a symbol of masculinity, strength, and power [18]. However, research suggests that penis loss does not necessarily negatively impact relationships and, in some situations, can improve them, including the development of satisfying intimate relationships [19]. The patient feared he might not meet cultural expectations of masculinity, so he was recommended reality therapy, during which the patient learns to recognize his needs and make appropriate decisions, leading to increased self-confidence, gaining internal control, and taking responsibility for his own actions [20].
A phantom erection is a consequence of the severing or loss of sensory receptors in the penis following amputation. However, their counterparts remain in the cerebral cortex, where they are activated by sexual desire, leading to the sensation of an erection [21]. Using mirror therapy can create a visual illusion of penis movement or retraction, which can provide a sense of control or relief. By manipulating the visual experience, a person can potentially alter their perception and control this illusion [22]. The patient declined mirror therapy, citing “no clear purpose to the therapy.” Alternatively, he was offered relaxation activities to distract him from the phantom erections, which yielded positive results.
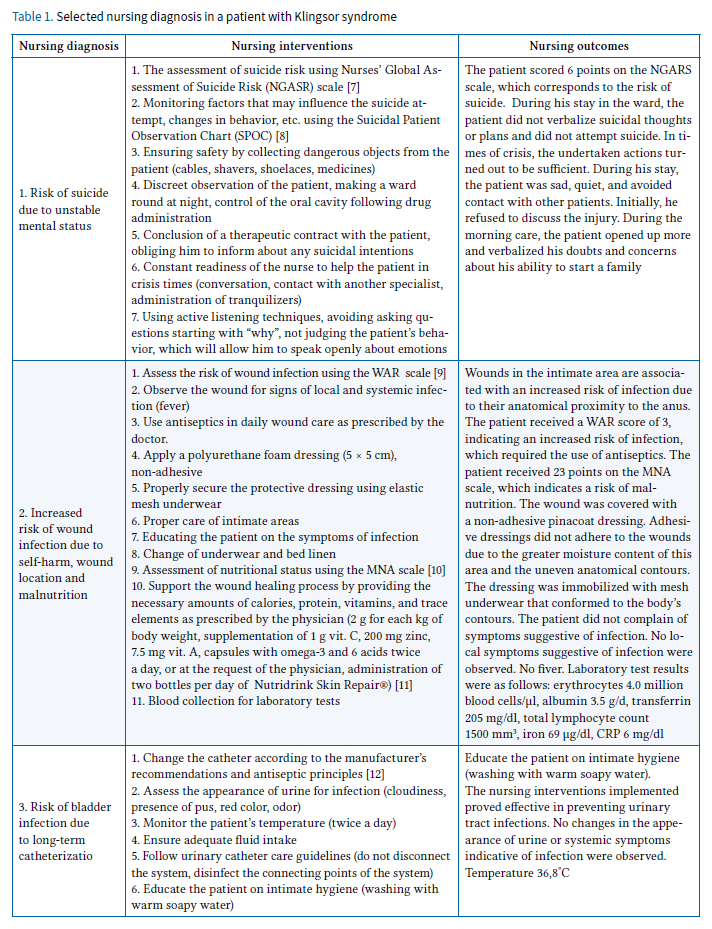
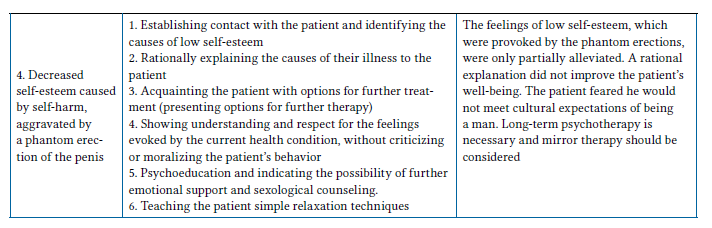
In the nursing process, the NANDA classification was used, the interventions were developed according to the Nursing Interventions Classification (NIC), and the results of care were rated according to the Nursing Outcomes Classification (NOC) [23].
The patient was diagnosed with the following nursing diagnoses (Table 1):
- Suicide risk. The goal of the intervention was to ensure patient safety and prevent suicide attempts.
- Increased risk of wound infection. Nursing interventions were aimed at minimizing the risk of wound infection and optimizing the healing process.
- Risk of bladder infection. The goal of nursing interventions was to prevent urinary tract infections.
- Reduced self-esteem. The goal of nursing care was to improve mood.
Conclusions
Penile self-harm is a rare but serious condition that carries long-term consequences for the patient. It requires the implementation of evidence-based nursing care and the involvement of multiple specialists, including surgeons, psychiatrists, and sexologists. The diversity of nursing problems poses a challenge for nurses caring for patients with Klingsor syndrome. It is important to consider the patient not only through the lens of wound care but also in the context of the psychosocial consequences of genital self-harm. Holistic patient care allows for the best outcomes and improved quality of life.
Disclosures
The author declares no conflict of interest. This research received no external funding. Approval of the Bioethics Committee was not required.
References
- Veeder TA, Leo RJ. Male genital self-mutilation: a systematic review of psychiatric disorders and psychosocial factors. Gen Hosp Psychiatry 2017; 44: 43–50. DOI: 10.1016/j.genhosppsych.2016.09.003.
- Roth K, Izard J, Beiko D. Self-performed glansectomy and surgical repair by a nonpsychotic patient on androgen replacement therapy. Can Urol Assoc J 2009; 3: 25–28. DOI: 10.5489/cuaj.1135.
- Odeyemi PO, Idowu NA, Abiola OO, Okunade IA. Genital self-mutilation following cannabis-induced psychosis: Klingsor syndrome – a case report. African Urology 2024; 4: 36–39. DOI: 10.36303/AUJ.0121.
- Mirastschijski U, Jiang D, Rinkevich Y. Genital Wound Repair and Scarring. Med Sci (Basel) 2022; 10: 23. DOI: 10.3390/medsci10020023.
- Mortada H, Alhablany T, Alkahtani D, et al. Meshed Versus Sheet Skin Graft for Scrotum and Perineal Skin Loss: A Retrospective Comparative Study. Cureus 2021; 13 (9). DOI: 10.7759/cureus.18348.
- Van der Merwe A, Graewe F, Zühlke A, et al. Penile allotransplantation for penis amputation following ritual circumcision: a case report with 24 months of follow-up. Lancet 2017; 390: 1038–1047. DOI: 10.1016/S0140-6736(17)31807-X.
- Grosse U, Pfister A, Zeyer A, Häusermann S. Klinisches Assessment Basiswissen für Pflegefachpersonen und Hebammen. Arbeitsheft Psychiatrie. Zürcher Hochschule für Angewandte Wissenschaften 2023.
- Björkdahl A, Nyberg U, Runeson B, Omérov P. The development of the Suicidal Patient Observation Chart (SPOC): Delphi study. J Psych Ment Health Nurs 2011; 18: 558–561. DOI: 10.1111/j.1365-2850.2011.01758.x.
- Sopata M, Jawień A, Mrozikiewicz-Rakowska B, et al. Wytyczne postępowania miejscowego w ranach niezakażonych, zagrożonych infekcją oraz zakażonych – przegląd dostępnych substancji przeciwdrobnoustrojowych stosowanych w leczeniu ran. Zalecenia Polskiego Towarzystwa Leczenia Ran. Leczenie Ran 2020; 1–21. DOI: 10.5114/lr.2020.96820.
- Cierzniakowska K, Szewczyk M, Kozłowska E, et al. Nutrition state assessment of elder patients hospitalised in a surgical ward. Pielęg Chir Angiol 2017; 11: 61–67.
- Wojda P. Chronic wound care in psychiatric nursing practice. A case study. Forum Leczenia Ran 2022; 3: 41–48. DOI: 10.15374/FLR2022026.
- Prävention und Kontrolle Katheter-assoziierter Harnwegsinfektionen. Empfehlung der Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO) beim Robert Koch-Institut. Bundesgesundheitsbl 2015; 58: 641–650. DOI: 10.1007/s00103-015-2152-3
- Velazquez N, Press B, Renson A, et al. Development of a Novel Prognostic Risk Score for Predicting Complications of Penectomy in the Surgical Management of Penile Cancer. Clin Genitourin Cancer 2019; 17: 123–129. DOI: 10.1016/j.clgc.2018.09.018.
- Efron DT, Barbul A. Wounds in infection and sepsis – role of growth factors and mediators. In: Holzheimer RG, Mannick JA (eds.). Surgical Treatment: Evidence-Based and Problem-Oriented. Zuckschwerdt, Munich 2001; 1–10.
- Myoungjean J, Yoonhong K, Kyung WS. Role of nutrition in wound healing and nutritional recommendations for promotion of wound healing: a narrative review. Ann Clin Nutr Metab 2023; 15: 67–71. DOI: 10.15747/ACNM.2023.15.3.6
- Willson M, Wilde M, Webb ML, et al. Nursing interventions to reduce the risk of catheter-associated urinary tract infection: part 2: staff education, monitoring, and care techniques. J Wound Ostomy Continence Nurs 2009; 36: 137–154. DOI: 10.1097/01.WON.0000347655.56851.04
- Alghamdi SA, Alahmari MA, Alenazy BA, et al. The Role of Nursing in Suicide Prevention: Evidence-Based Practices, Challenges, and Future Directions. Review of Contemporary Philosophy 2023; 22: 1044–1063.
- Santos DD, Carneiro S, Corrêa RG. Nursing care and sexuality in Oncology for penectomized individuals. Revenferm UERJ, Rio de Janeiro 2023; 31. DOI: 10.12957/reuerj.2023.68807.
- Sosnowski R, Kulpa M, Kosowicz M, et al. Quality of life in penile carcinoma patients – post-total penectomy. Cent European J Urol 2016; 69: 204–211. DOI: 10.5173/ceju.2016.828.
- Karimyar Jahromi M, Mosallanejad L. The impact of reality therapy on metacognition, stress and hope in addicts. Glob J Health Sci 2014; 6: 281–287. DOI: 10.5539/gjhs.v6n6p281.
- Namba Y, Sugiyama N, Yamashita S, Tokuyama E, Hasegawa K, Kimata Y. Phantom erectile penis after sex reassignment surgery. Acta Medica Okayama 2008; 62: 213–216. DOI: 10.18926/AMO/30981.
- Ramachandran VS, McGeoch PD. Phantom penises in transsexuals: Evidence of an innate gender-specific body image in the brain. J Conscious Stud 2008; 15: 5–16.
- Ackley BJ, Ladwig GB (eds.). Podręcznik diagnoz pielęgniarskich. Media House, Warszawa 2019.