Opis przypadku | Case report
The use of split-thickness skin grafts and negative pressure wound therapy in the treatment of lower limb frostbite
Jakub Boryczko![]() 1,2, Bogusław Strzałko1, Dariusz Bazaliński
1,2, Bogusław Strzałko1, Dariusz Bazaliński![]() 1,3
1,3
1 Specialist Hospital Podkarpackie Oncology Center, Brzozow, Poland
2 Jan Grodek State University in Sanok, Poland
3 Faculty of Health Sciences and Psychology, University of Rzeszow, Poland
Address for correspondence: Jakub Boryczko, Szpital Specjalistyczny Podkarpacki Ośrodek Onkologiczny, Brzozow, 18 Księdza Józefa Bielawskiego St., 36-200 Brzozow, Poland, e-mail: jakub.boryczko@icloud.com
Received: 11.08.2025 Accepted: 23.09.2025
LECZENIE RAN 2025; 22 (3): 115–121
DOI: https://doi.org/10.60075/lr.v22i3.112
Spis treści:
Abstract
Introduction
Material and methods
Case description
Discussion
Conclusions
Disclosures
References
Abstract
Introduction: Soft tissue damage in the form of difficult-to-heal wounds is a common complication of frostbite of the distal parts of the body. Changes in the tissues impair microcirculation and disrupt regenerative processes. Selecting the appropriate treatment based on physical assessment and additional specialist tests improves the patient’s condition, reduces the number of complications, and speeds up recovery.
Aim of the study: To present the treatment process for frostbite of the lower limbs resulting from exposure to adverse weather conditions.
Material and methods: A case study method was used in this study. The study design was based on the CARE guidelines. A 64-year-old woman who was being treated for paranoid schizophrenia presented with third-degree frostbite on her shins and feet. Due to her refusal to undergo amputation, necrotic tissue was excised several times, free split-thickness skin grafts were performed, and negative pressure wound therapy (NPWT) was applied. The treatment resulted in a good therapeutic effect and recovery.
Results: The treatment and care measures were aimed at controlling the developing infection, managing the wound professionally, restoring repair processes, restoring skin continuity, and minimising pain. The entire therapeutic process took place at the General Surgery Department in an inpatient setting. Controlling the infection through empirical and targeted antibiotic therapy, as well as excising the necrotic tissue that was the source of the infection, allowed the wound to be debrided and prepared for skin grafting. NPWT accelerated the healing process. Intensive rehabilitation and early mobilisation allowed the patient to regain function in her lower limbs.
Conclusions: The use of free skin grafts and NPWT in the treatment of frostbite wounds shortens the hospital stay and accelerates the healing process.
Key words: skin graft, negative pressure wound therapy, injury, wound treatment, frostbite
Introduction
Frostbite is an injury to the soft tissues caused by exposure to low temperatures. Tissue damage can occur when exposed to temperatures below –0.5°C. Frostbite occurs when exposure is long enough for the water in the tissues to form ice crystals, which result in frostbite injuries [1]. Injuries that do not involve the formation of ice crystals (non-freezing cold injuries) are also classified. Functional changes that result in non-freezing tissue damage, both local and general, are caused by low ambient temperatures. Non-freezing injuries are referred to as chilblains, also known as frostbite, and hypothermia can occur when exposed to atmospheric conditions with temperatures between 0 and 16°C, usually in a cold, dry, or humid environment for several hours. Exposure to low temperatures can lead to systemic hypothermia, which poses a risk of serious health consequences [2].
The process of cooling the skin causes the blood vessels to constrict and then dilate periodically. When the skin is rewarmed, the injury leads to inflammation, constriction of blood vessels, thrombosis, vascular obstruction, blistering, and ultimately tissue damage and necrosis [3]. Most thermal injuries can be avoided by wearing appropriate clothing and limiting exposure to low temperatures. For people who have suffered tissue frostbite, early intervention to prevent tissue damage is essential. The treatment process is lengthy. Patients with extensive frostbite require long-term professional care. In some cases, amputation is necessary. Frostbite is associated with numerous risk factors. The most significant ones are homelessness and low socioeconomic status, alcohol abuse, smoking, mental disorders, and addiction to psychoactive substances. Personal factors have also been identified, including inadequate or inappropriate winter clothing, delay in seeking medical assistance, and lack of knowledge about how to behave in cold conditions [4]. Alcohol and other psychoactive substance abuse are among the factors that increase the risk of amputation [5]. Complications of frostbite place a significant burden on the healthcare system due to costly procedures and long hospital stays [6].
In Central Europe, low temperatures cause about 35 times fewer thermal injuries than burns. Their treatment is not standardised, and there is no algorithm for managing patients who have suffered frostbite. Therefore, it is largely based on case reports, clinical observations, and experience from other centres. The treatment of injuries caused by low temperatures depends on the type and severity of the injury, as well as the time of treatment initiation. In Europe, this group of patients is treated in burn units and surgical wards [7].
Prolonged healing of frostbite wounds resulting from progressive inflammation and tissue ischemia leads to extensive scarring and limited joint mobility. This causes significant physical impairment and reduces patients’ quality of life. Secondary malignant tumours may also develop as a result. Consequently, modern wound treatment methods are of great importance [8].
This study aims to present treatment methods for hard-to-heal wounds caused by low temperatures.
Material and methods
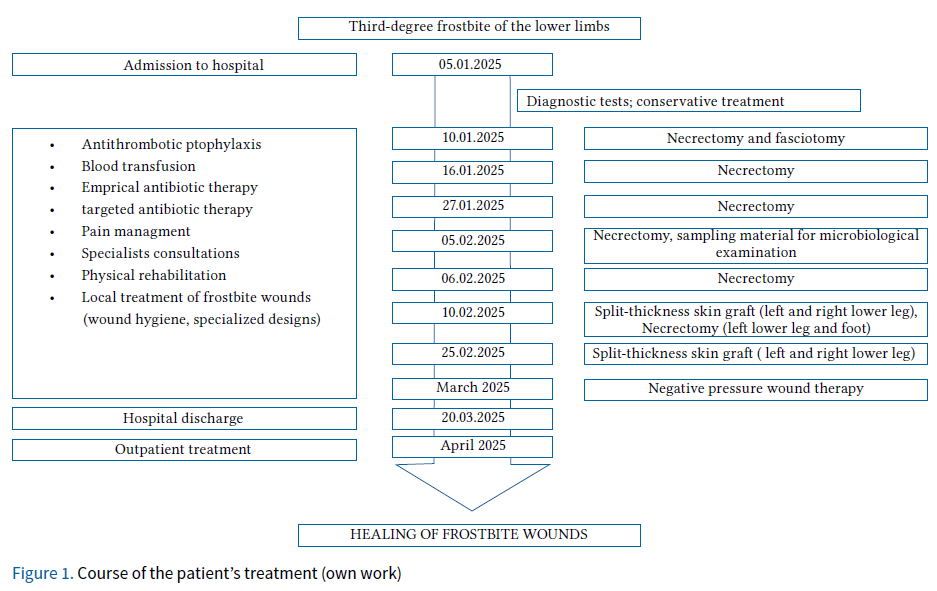
The case study method was used. The study design was based on the CARE guidelines. The patient was a 64-year-old woman treated for paranoid schizophrenia, who also had third-degree frostbite of the shins and feet. In the absence of consent for amputation, necrotic tissue was excised several times, free split-thickness skin grafts were performed, and negative pressure wound therapy (NPWT) was applied. The treatment resulted in a positive therapeutic outcome and recovery. Observation, interview, and analysis of medical records were conducted in a hospital setting from January 2025 to April 2025. During this time, necrotic tissue was repeatedly removed, skin grafts were performed, and NPWT was administered. Systemic treatment was also used to control the developing infection, prevent thrombosis, and provide multimodal pain management. The head of the department authorised the study, and the patient consented to the publication of photos upon discharge. The entire research process was conducted in accordance with the guidelines of the Declaration of Helsinki [9]. The treatment process is presented in Figure 1.
Case description
A 64-year-old woman, previously independent in terms of self-care and self-support, diagnosed with paranoid schizophrenia, was admitted after being transferred by the Emergency Medical Services on 5 January 2025 to the Specialist Hospital in Brzozow, General Surgery Ward, due to third-degree frostbite of both shins and feet.
The patient reported walking in the snow for several hours in low temperatures without shoes. Upon admission, she was alert, oriented to self, and allopsychic, exhibiting inappropriate affect and a depressed mood. A local examination revealed cold limbs with damaged skin on the feet and the lower parts of both shins. The tissue damage covered approximately 18% of the total body surface area. The pulse was weak, and sensation was impaired with signs of hyperalgesia. The tissue damage was initially classified as second- to third-degree frostbite (Fig. 2). There was a full-thickness skin wound on the right foot suggesting ulceration. Initial treatment was administered, and tissue biopsies were taken for microbiological evaluation. Laboratory tests showed signs of inflammation: C-reactive protein (CRP): 9.01 (0–5 mg/l), procalcitonin (PCT): 840 (150–400; 10³/mm³), anaemia: hemoglobin (HGB): 7.4 g/dl (13.7–16.5 g/dl), and hematocrit (HCT): 22.2% (40.1–51.0%). The patient received 2 units of red blood cell concentrate, and the blood morphology normalised: HGB: 11.5 g/dl (13.7–16.5 g/dl), HCT: 35.4% (40.1–51.0%). The patient received observation, multimodal pain management, and local wound care. Over the next few days, conversion associated with deepening tissue damage, and spreading necrosis was observed. Doppler ultrasound of the lower extremities confirmed preserved vascular flow in the peripheral arteries. On the fifth day of hospitalisation, an increase in inflammatory parameters (CRP: 296 mg/l) was observed due to a developing infection originating from necrotic tissue in the lower legs and feet. Empirical antibiotic therapy was initiated, involving amoxicillin with clavulanic acid. Amputation of both lower limbs was proposed on life-saving grounds, pointing to critical skin damage and the risk of sepsis. However, the patient did not consent to this procedure. The consulting psychiatrist found her to be fully conscious and capable of making decisions. Over the next few days, the patient maintained her position regarding her refusal to undergo surgery.
The patient was referred to the operating room for a necrectomy and fasciotomy due to life-threatening fascial compartment syndrome in both lower limbs (Fig. 3). The necrotic tissue was removed, exposing the healthy muscle. A microbiological examination of the tissue biopsy revealed the presence of the following aerobic bacteria: Escherichia coli, Providencia rettgeri, Acinetobacter baumannii, and Enterococcus faecalis. Based on the antibiogram, targeted treatment with cloxacillin and cotrimoxazole was initiated. In the days that followed, a drop in inflammatory markers was seen (CRP: 173 mg/l [0–5 mg/l] on the third day after surgery and 143 mg/l [0–5 mg/l] on the fifth day).
On day 11 of hospitalisation (Fig. 4), further excision of necrotic tissue was performed in the operating room, and material was collected again for microbiological examination. Follow-up laboratory tests performed on day 13 of hospitalisation revealed a decrease in CRP to 113 mg/l (normal range: 0-5 mg/l).
On day 15 of hospitalisation, further removal of necrotic tissue was performed in the operating room. Systematic removal of necrotic tissue and targeted antibiotic therapy resulted in a decrease in acute phase protein concentrations. Follow-up tests revealed a subsequent decrease in CRP levels, from 55 mg/l to 34 mg/l. Follow-up blood cultures were also performed with negative results. Additional tests were performed as part of further diagnostics, confirming a positive test result for Borrelia burgdorferi bacteria. A neurologist consulted the patient and additionally diagnosed neuroborreliosis.
On day 30 of hospitalisation (Fig. 5), a second necrectomy was performed in the operating room, and tissue samples were collected for microbiological examination. These samples yielded cultures of Staphylococcus aureus and Acinetobacter baumannii strains. Because both strains were sensitive to gentamicin, intravenous gentamicin was administered while monitoring the gentamicin concentration in the blood. The ward systematically changed polyhexanide and povidone-iodine dressings, as well as paraffin mesh dressings. Gradual cleansing of the frostbite wounds was achieved.
On 10 February 2025 a free split-thickness skin graft was placed on the left shin and ankle area (Fig. 6) using a 1 : 3 mesh. The graft was secured with 3-0 absorbable sutures. Both the grafted mesh and the donor site were covered with a paraffin dressing. Another necrectomy was performed on the right lower limb and secured with an iodine-povidone dressing and antiseptic gel containing surfactant. There were no problems with wound healing at the donor site (thigh). During hospitalisation, the patient underwent physical rehabilitation. Due to anaemia (HGB: 8 g/dl [normal range: 13.7–16.5 g/dl]; HCT: 26.1% [normal range: 40.1–51.0%]), 2 more units of red blood cell concentrate were transfused.
On 25 February 2025, additional split-thickness skin grafts were performed (Fig. 7). A 0.3-mm-thick skin flap was harvested from the donor site on the left thigh and placed on the left foot. Two flaps from the donor site on the right thigh were placed on the dorsal part of the right foot and the right lower leg. The grafts and donor sites were secured with a paraffin-impregnated mesh dressing.
A follow-up microbiological examination (biopsy from the wound) was performed on 28 February 2025. The following microorganisms were cultured: E. coli, S. aureus, A. baumannii, E. faecalis, P. multocida, and B. fragilis. The patient continued to receive targeted antibiotic therapy, which led to a decrease in CRP concentration to 20.8 mg/l. Physical rehabilitation and verticalisation of the patient were also continued. A psychological consultation was also performed. Over the next few days, NPWT at 80–120 mmHg was administered, which resulted in the skin grafts healing satisfactorily.
On 20 March 2025, the patient was discharged to a nursing home in satisfactory general and local condition to receive further outpatient treatment at the hospital’s Wound Treatment Clinic (Fig. 8).
Discussion
The presented case of a patient with difficult-to-heal wounds resulting from thermal injury to the lower limbs demonstrates a multidirectional and time-consuming therapeutic process that is supervised by an interdisciplinary team of specialists. The need to take the risk of local treatment and provide holistic care created opportunities for radical measures, which resulted in therapeutic success. The measures taken prevented amputation, and local treatment was carried out in accordance with the Polish Wound Treatment Society’s current guidelines. In addition to measures aimed at restoring function, the treatment included the TIMERS strategy, wound hygiene, and infection prevention with minimal antibiotic therapy [10, 11].
Frostbite of the lower limbs is associated with a significant risk of amputation, which increases with the area and depth of tissue damage [12]. Additionally, soft tissue oedema resulting from inflammatory mediators, vasomotor disorders, and thrombotic changes can cause compartment syndrome. This condition can lead to secondary acute ischaemia and amputation of the limb [13].
The patient refused to consent to the amputation of her limbs as proposed by the doctors on duty in the general surgery ward, so the initial course of treatment was determined by this refusal. This decision was made based on the condition of the limbs, but also on the potential difficulties associated with self-care and making rational decisions related to the course of mental illness. Given the situation, conservative treatment was initiated during the first days of hospitalisation to control the developing infection and treat the frostbite wounds. During this period, additional tests were performed to evaluate blood flow to the limbs. On day 5 of hospitalisation, with the support of a psychiatrist and basic psychotherapy, the patient consented to a necrectomy in the operating room. Due to the risk of fascial compartment syndrome caused by severe soft tissue oedema, fasciotomy was also performed.
During the subsequent days of hospitalisation, additional necrosectomies were performed in the operating room to gradually eliminate the source of infection. Targeted antibiotic therapy was also administered. Microbiological assessment of the wound is important for controlling the infection. Due to the colonisation of the wound with bacteria, it is recommended that the appearance of the wound be observed for signs of local infection. The use of moist therapy in conjunction with autolytic wound cleansing was avoided due to the potential risk of infection from non-demarcated dead tissue. The use of PVP-I preparations allowed the wound to be maintained without liquefied necrotic tissue and reduced the duration of antibiotic therapy.
Proper collection of materials for microbiological testing and analysis of the antibiogram are essential for microbiological diagnosis and selecting the appropriate antibiotic [10]. Targeted antibiotic therapy was used during treatment until markers of inflammation decreased to levels that did not pose a risk of systemic infection. This therapy was combined with local wound treatment, including irrigation with antiseptics and lavaseptics, scraping, and specialised dressings containing polyhexamethylene biguanide and iodopovidone, which penetrates deeply into tissues and exhibits effective antimicrobial activity [8].
The treatment significantly improved the local condition and decreased the concentration of acute phase proteins. Rapid repair processes and gradual formation of granulation tissue were observed in the wounds. In the next stage of treatment, free split-thickness skin grafts were used to cover the patient’s frostbite wounds. The grafts were taken from donor sites on the thighs. Before a skin graft can be performed, the wound must be properly prepared. In addition to preparing the granulating wound bed, which increases the chances of graft acceptance, it is important to treat the wound edges. One way to do this is to excise the wound edges before the graft, which causes the release of cytokines and inflammatory mediators. Additionally, the wound must be free of microorganisms and necrotic tissue that blocks the ingrowth of blood vessels into the graft. Skin grafts currently play a key role in modern wound treatment and tissue regeneration. Although autologous split-thickness skin grafts (STSGs) are considered the gold standard for treating chronic limb ulcers due to their safety and efficacy, their use may be limited in practice by patient factors such as fear of failure, larger wound formation, reluctance to be hospitalised, limited access to professional care, and insufficient knowledge about the method [13]. Proper wound preparation for skin grafting requires optimisation of all patient-related factors and allows for favourable outcomes [14].
The next stage of treatment involved the use of local NPWT. Negative pressure wound therapy is a safe and effective treatment method that promotes skin graft healing more effectively than traditional dressings [15]. Negative pressure achieves an 8.3% higher overall graft acceptance rate, and using the optimal value of –80 mmHg increases this rate by 10% [16]. Using controlled negative pressure reduces the risk of graft rejection and reoperation, as well as reducing treatment costs by shortening hospital stays and decreasing complications. Additionally, skin grafts are well reimbursed by insurers, and the overall hospitalisation cost is less than that of amputations [17].
In summary, the positive therapeutic outcome was achieved through the use of appropriately selected debridement methods, fasciotomy, multistage necrectomy, skin grafts, NPWT, and wound management concepts, as well as the selection of specialised dressings according to current guidelines and adaptation to the patient’s preferences and comfort. Thanks to the interdisciplinary team’s efforts, the patient regained her mobility.
Conclusions
Free split-thickness skin grafts significantly shorten the healing time of frostbite wounds in the lower extremities. The use of local NPWT accelerates the ingrowth of the grafted epidermis. The treatment in question has been shown to enhance patients’ quality of life and reduce wound healing time, leading to an overall reduction in treatment costs.
Disclosures
The authors declare no conflict of interest. This research received no external funding. Approval of the Bioethics Committee was not required.
References
- Loren Lorentzen AK, Davis C, Penninga L. Interventions for frostbite injuries. Cochrane Database Syst Rev 2020; 12: CD012980. DOI: 10.1002/14651858.CD012980.pub2.
- Regli IB, Strapazzon G, Falla M, Oberhammer R, Brugger H. Long-Term Sequelae of Frostbite-A Scoping Review. Int J Environ Res Public Health 2021; 18: 9655. DOI: 10.3390/ijerph18189655.
- Wroñski K, Bocian R. Treatment of frostbites. Pielęg Chir Angiol 2010; 4: 114–118.
- Essien SK, Chireh B, Steinberg C, Omondi P, Zucker-Levin A. Psychosocial and personal predisposing factors of frostbite injury and associated amputation: a systematic review. Inj Epidemiol 2024; 11: 62. DOI: 10.1186/s40621-024-00546-w.
- Dow J. Cold Injury. Emerg Med Clin North Am 2024; 42: 513–525. DOI: 10.1016/j.emc.2024.02.012.
- Endorf FW, Alapati D, Xiong Y, et al. Biopsychosocial factors associated with complications in patients with frostbite. Medicine (Baltimore) 2022; 101: e30211. DOI: 10.1097/MD.0000000000030211.
- Sachs C, Lehnhardt M, Daigeler A, Goertz O. The Triaging and Treatment of Cold-Induced Injuries. Dtsch Arztebl Int 2015; 112: 741–747. DOI: 10.3238/arztebl.2015.0741.
- Wang W, Liu P, Zhu W, et al. Skin organoid transplantation promotes tissue repair with scarless in frostbite. Protein Cell 2025; 16: 240–259. DOI: 10.1093/procel/pwae055.
- World Medical Association. Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects. Available at: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (Access: June 15, 2025).
- Sopata M, Jawieñ A, Mrozikiewicz-Rakowska B, et al. Guidelines for local management of uninfected, infection-prone, and infected wounds – a review of available antimicrobial agents used in wound treatment. Recommendations of the Polish Wound Treatment Society. Leczenie Ran 2020; 17: 1–21.
- Moœcicka P, Cwajda-Bia³asik J, Jawieñ A, et al. Wound hygiene in the care of patients with lower limb ulceration. A description of three clinical cases. Leczenie Ran 2021; 18: 57–64. DOI: 10.5114/lr.2021.107150.
- Menon V, Richards L, Walter C, et al. Patient and treatment characteristics that predict symptom resolution and limb amputation in patients with frostbite. Burns 2025; 51: 107547. DOI: 10.1016/j.burns.2025.107547.
- Serra R, Rizzuto A, Rossi A, et al. Skin grafting for the treatment of chronic leg ulcers – a systematic review in evidence-based medicine. Int Wound J 2017; 14: 149–157. DOI: 10.1111/iwj.12575.
- Brandão RA, St John JM, Langan TM, Schneekloth BJ, Burns PR. Acute Compartment Syndrome of the Foot Due To Frostbite: Literature Review and Case Report. J Foot Ankle Surg 2018; 57: 382–387. DOI: 10.1053/j.jfas.2017.07.005.
- Gorka R. Preparation for a Successful Skin Grafting. In: Skin Grafts for Successful Wound Closure [Internet]. IntechOpen 2022.
- Lee SC, Bayan L, Sato A, et al. Benefits of negative pressure wound therapy in skin grafts: A systematic review and meta-analysis of randomised controlled trials. J Plast Reconstr Aesthet Surg 2025; 102: 204–217. DOI: 10.1016/j.bjps.2025.01.03.
- Ker H, Al-Murrani A, Rolfe G, Martin R. WOUND Study: A Cost-Utility Analysis of Negative Pressure Wound Therapy After Split-Skin Grafting for Lower Limb Skin Cancer. J Surg Res 2019; 235: 308–314. DOI: 10.1016/j.jss.2018.10.016.